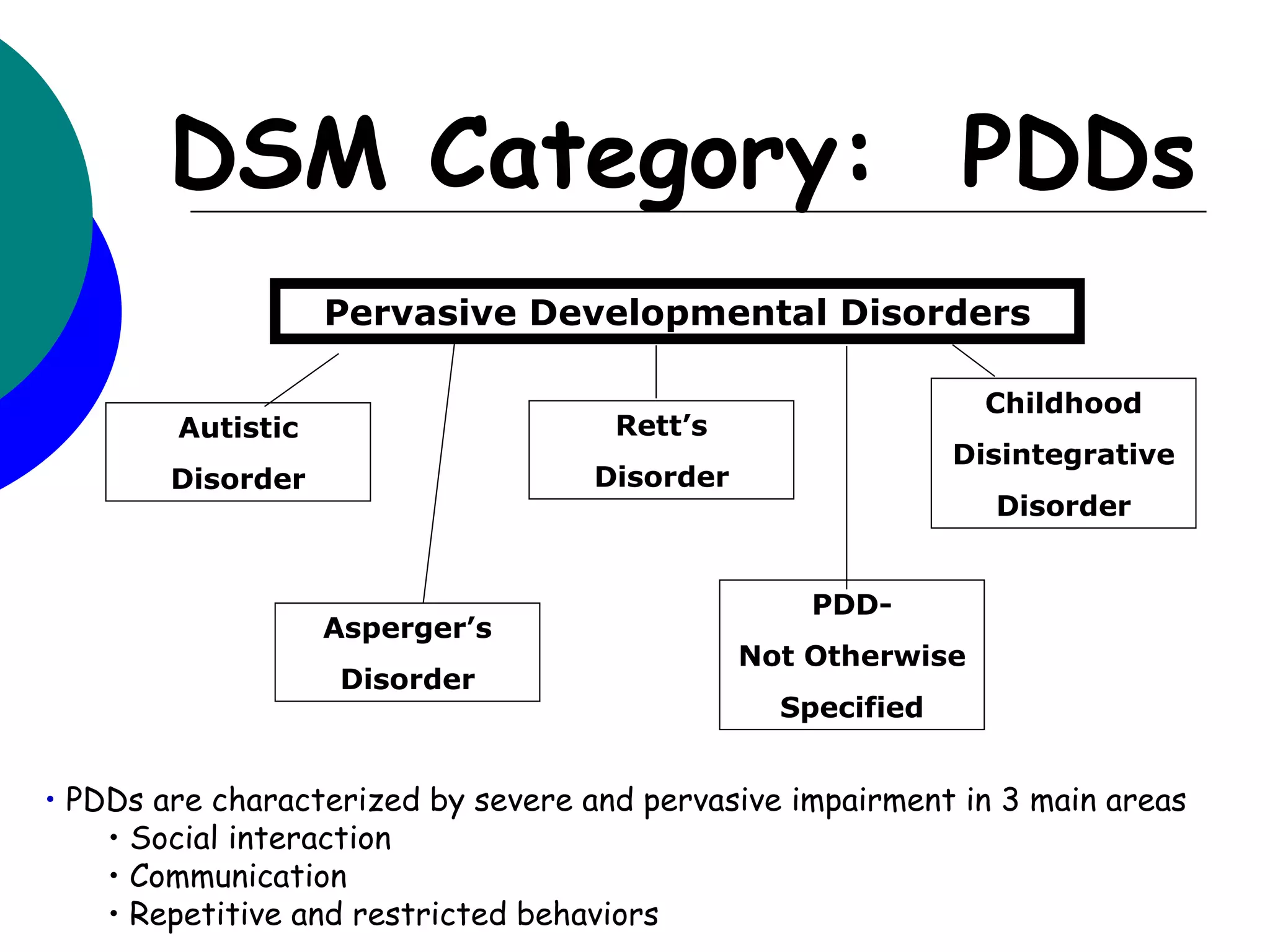
The document provides a history of autism including its original use by Bleuler in 1911 and further definition by Kanner in 1943. It discusses research and definitions by Asperger, Eisenberg, Creak, and Rutter that helped characterize autism. The Diagnostic and Statistical Manual of Mental Disorders (DSM) included autism for the first time in 1980 and further defined pervasive developmental disorders. The DSM-IV criteria require impairments in social interaction, communication, and repetitive behaviors. Prevalence of autism has increased since first measured in 1966, estimated now at 1 in 150 children. Boys are 4 times more likely to be affected than girls.