Downloaded 94 times

![Nuss Procedure
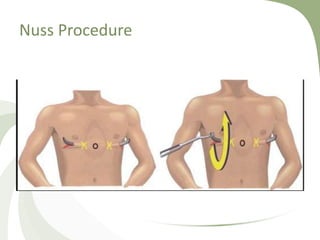
• Nuss procedure (aka minimally invasive repair of pectus
excavatum [MIRPE]) — closed procedure that corrects the
pectus defect without cartilage resection by applying outward
pressure to the sternum at the point of maximal inward
deflection using a custom- contoured steel bar ("Nuss bar”)
• The Nuss bar is placed in the pleural space, passed behind the
sternum, rotated 180 degrees, and then attached laterally to
the outer edge of the rib cage. The bar is left in place for
several months or years.](https://image.slidesharecdn.com/finalchestwall-180805194312/85/Congenital-Chest-Wall-Abnormality-21-320.jpg)
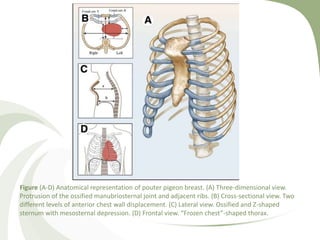
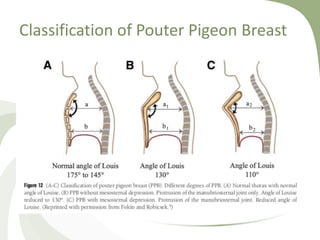

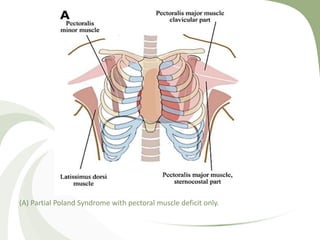
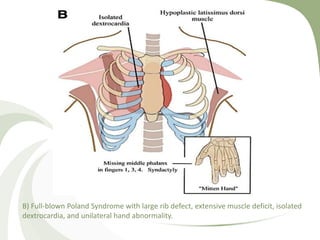
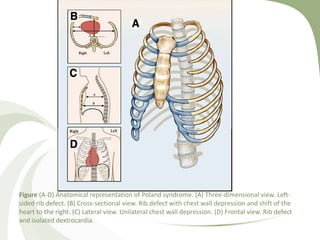

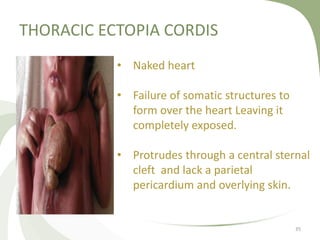
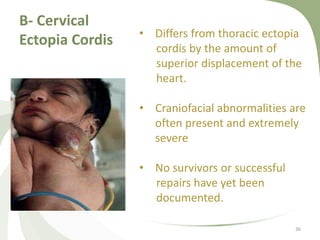
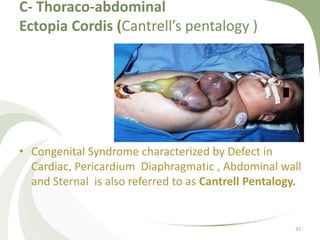
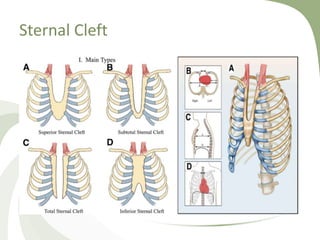
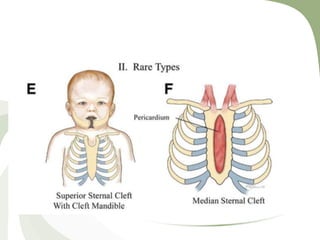


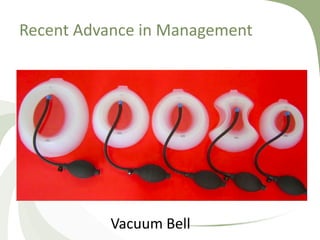





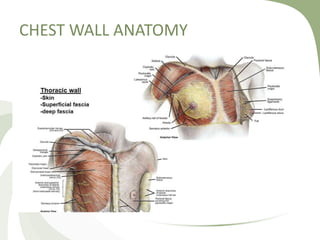
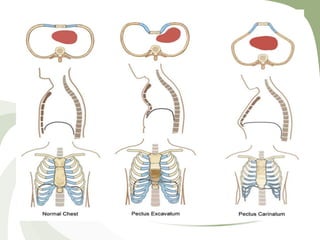
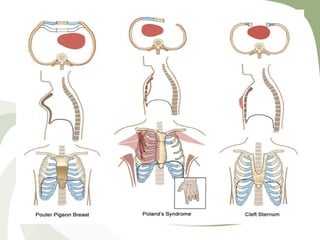
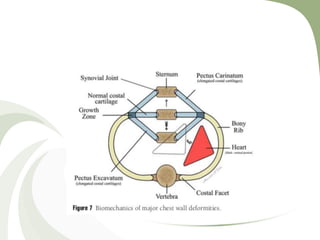
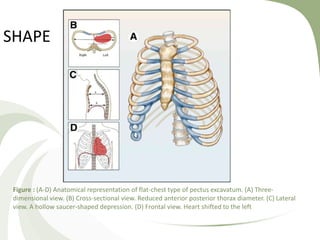
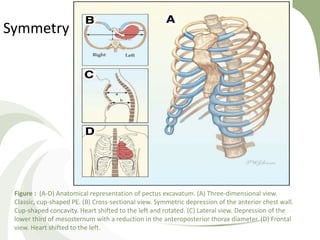
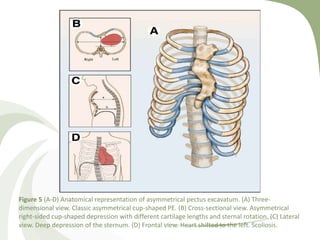
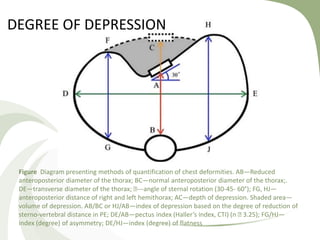
This document provides an overview of congenital chest wall abnormalities, including the anatomy and development of the chest wall. It outlines several common chest wall deformities such as pectus excavatum, pectus carinatum, Poland's syndrome, ectopia cordis, and bifid sternum. For each condition, it describes the clinical presentation, classification, and current treatment approaches. The document concludes by mentioning recent advancements in management, including the vacuum bell, magnetic mini-mover procedure, and dynamic compression bracing.











































































