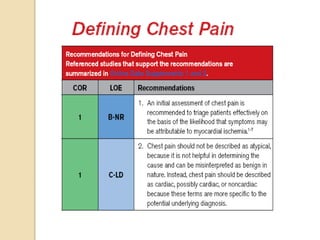
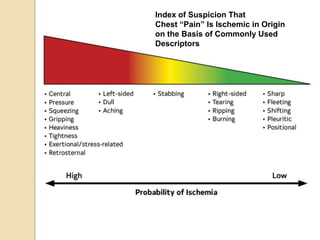
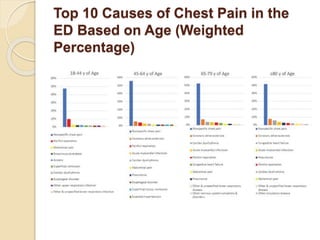
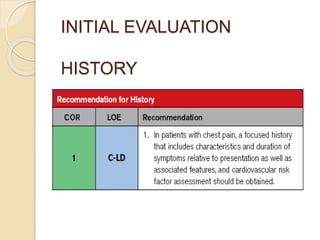
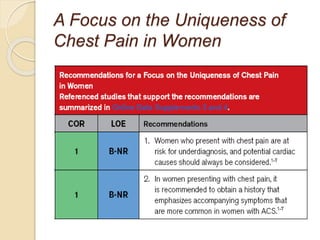
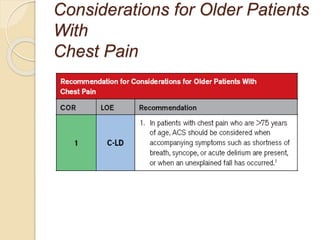
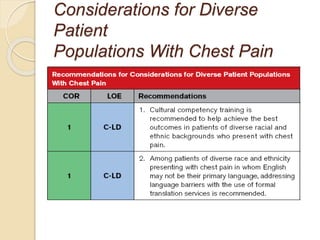
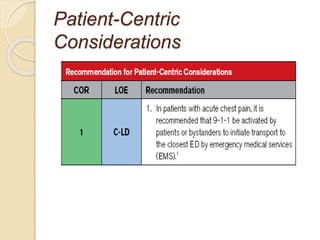
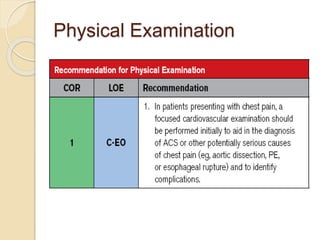
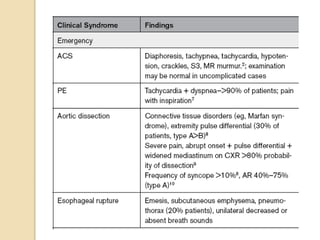
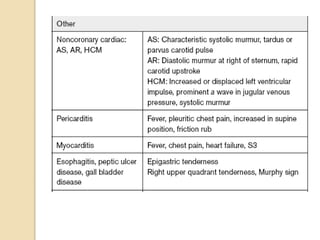
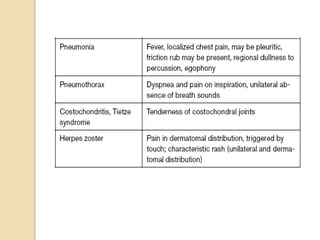
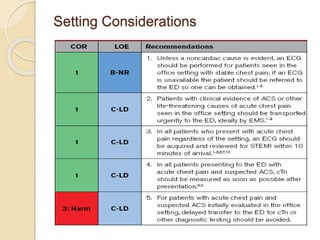
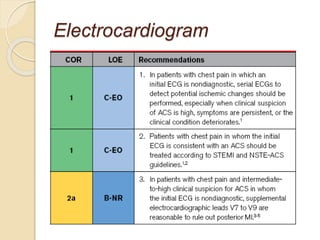
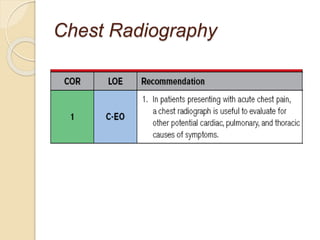
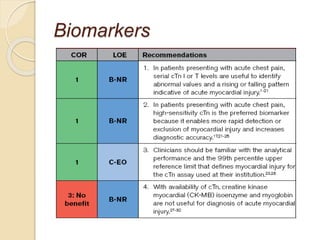
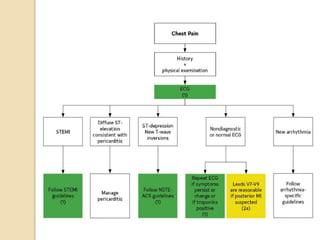
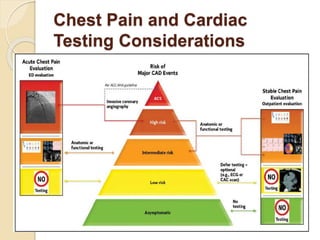
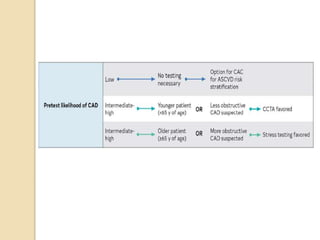
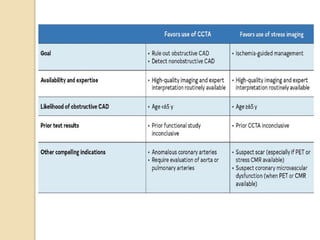
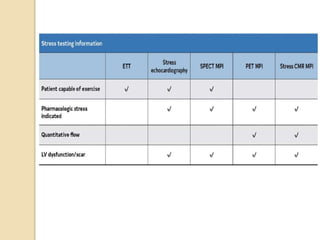
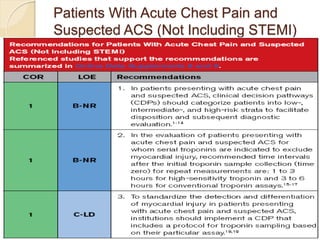
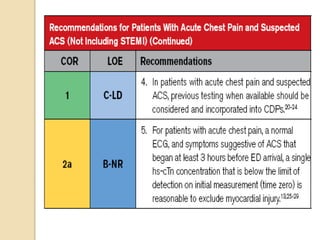
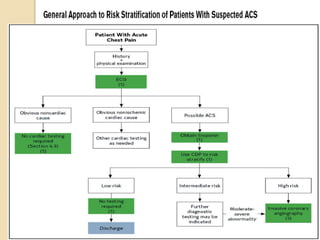
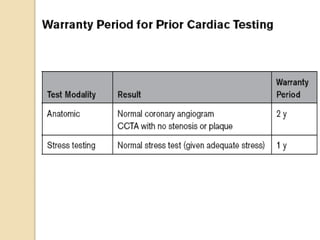
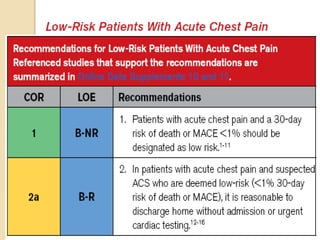
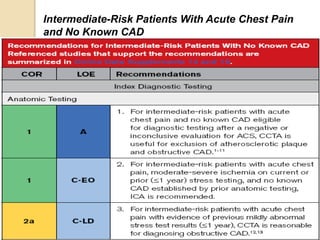
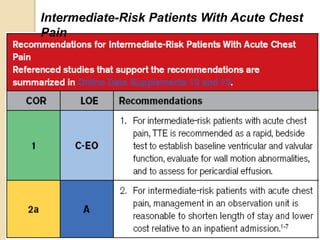
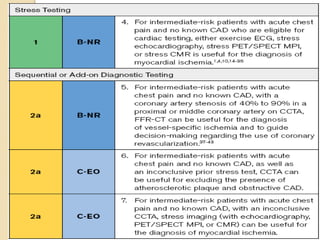
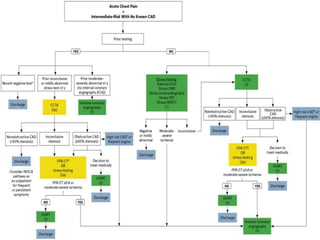
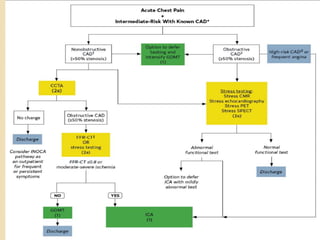
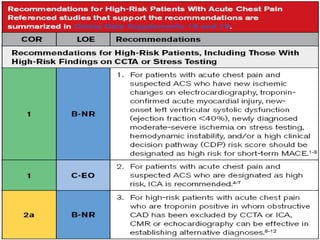
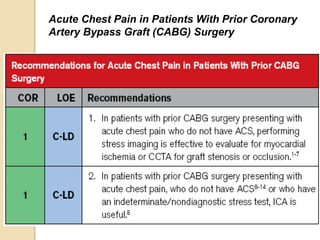
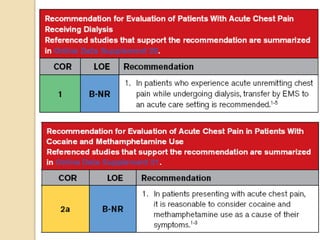
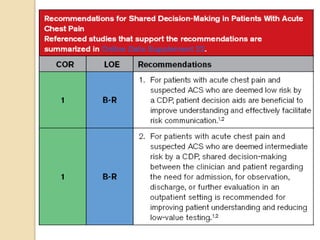
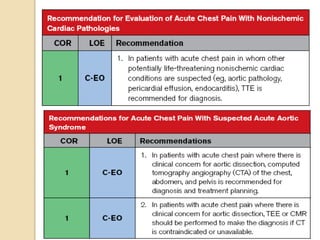
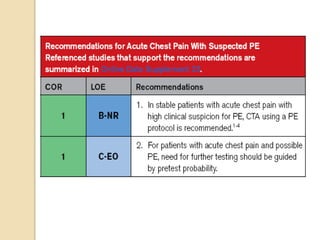
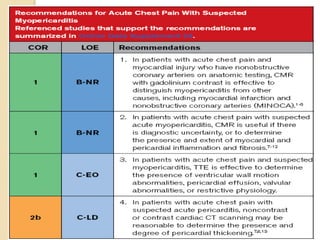
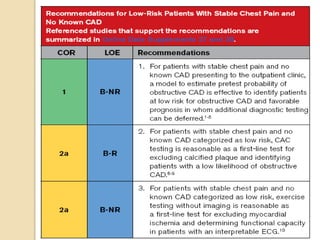
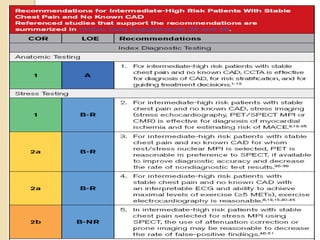
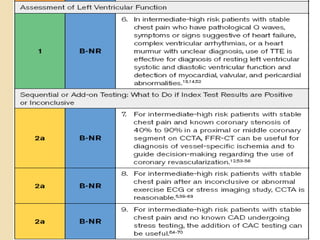
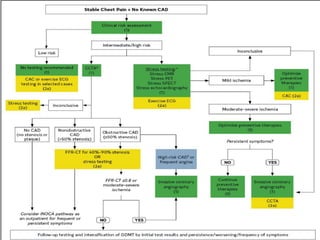
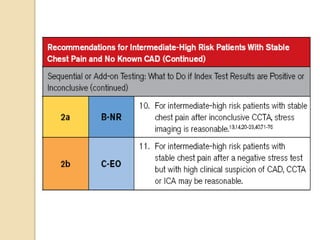
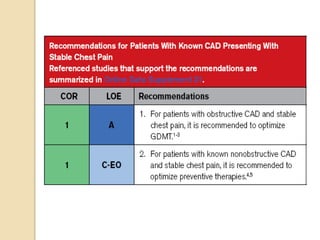
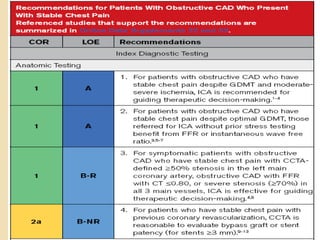
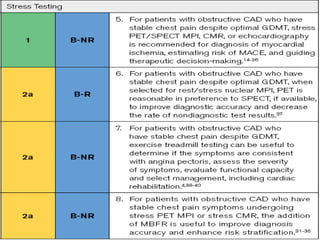
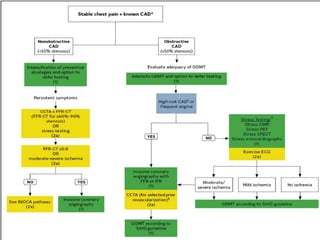
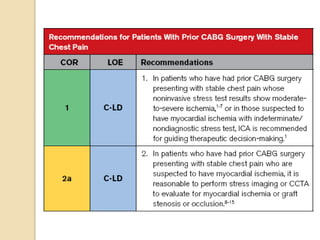
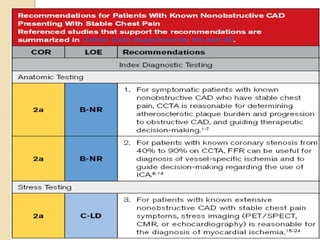
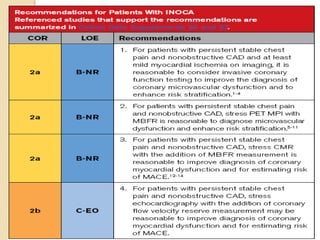
- The document summarizes guidelines for evaluating and diagnosing chest pain, including characteristics of cardiac vs. non-cardiac chest pain, initial evaluation involving history and physical exam, diagnostic testing considerations, and management strategies for patients with acute chest pain and suspected acute coronary syndrome (ACS) at different risk levels. Key points addressed include nature, location, precipitating/relieving factors of chest pain types, ECG and biomarker use, and testing algorithms for intermediate-risk patients both with and without known coronary artery disease.