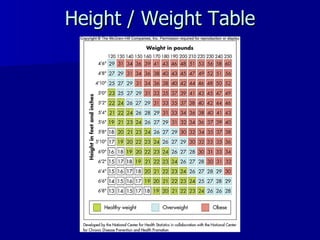
This document provides an overview of energy balance and weight control. It discusses factors that influence basal metabolism and physical activity, and how they impact energy needs and expenditure. The document estimates calorie needs and defines healthy versus unhealthy body weights using BMI. It also examines causes of obesity and strategies for successful weight loss and maintenance through calorie control, physical activity, and behavior modification.