Downloaded 59 times
![Reference
O Stefan Engeli; “The clinical pharmacology of obesity”, Therapeutic Advances in Endocrinology and
Metabolism (2012) 3(3) 83–84
O Lee M. Kaplan, “Pharmacological Therapies for Obesity”, Gastroenterol Clin N Am 34 (2005) 91–104
O Obesity The Science Inside, book by American Association for the Advancement of Science.
O Stern J, Kazaks A, “ Obesity A Reference Handbook” 2009, Library of Congress Cataloging-in-
Publication Data, California
O Magdalena Warchoł, Hanna Krauss, Małgorzata Wojciechowska, Tomasz Opala, Beata Pięta, Wioletta
Żukiewicz-Sobczak, Justyna Kupsz, Alina Grochowalska “The role of ghrelin, leptin and insulin in
foetal development” Annals of Agricultural and Environmental Medicine 2014, Vol 21, No 2, 349–352
O G W Kim, J E Lin, E S Blomain, S A Waldman (2013). Antiobesity Pharmacotherapy: New Drugs and
Emerging Targets. [ONLINE] Available at:
http://www.nature.com/clpt/journal/v95/n1/fig_tab/clpt2013204t2.html#figure-title. [Last Accessed 10
November 2014 ].
19](https://image.slidesharecdn.com/obesity-141113003907-conversion-gate02/85/Obesity-19-320.jpg)

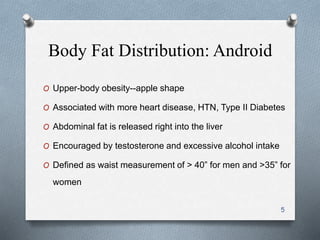
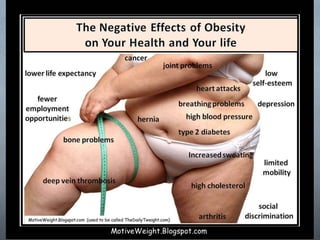
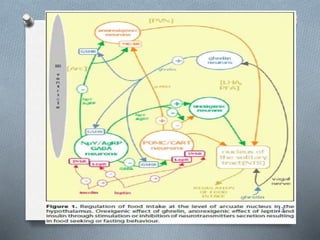
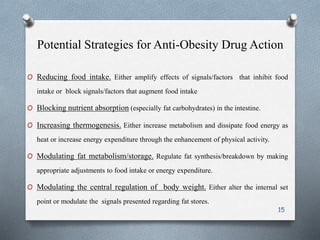
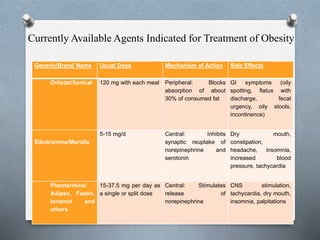
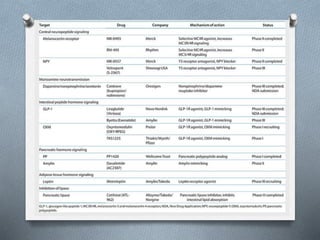
This document discusses obesity as the disease of the 21st century. It describes regional fat distribution patterns and their health risks, and explores the pathophysiology of obesity, including components of energy expenditure, the roles of brain neurotransmitters and hormones in regulating body weight. Finally, it examines current anti-obesity drugs like Orlistat, Sibutramine, and Phentermine that work by reducing nutrient absorption, inhibiting neurotransmitter reuptake, or stimulating norepinephrine release respectively, and considers future perspectives for obesity treatment.



























































































