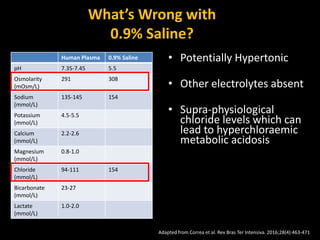
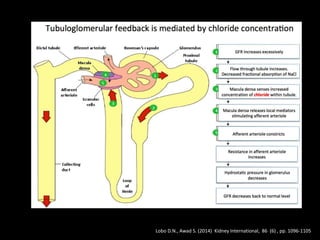
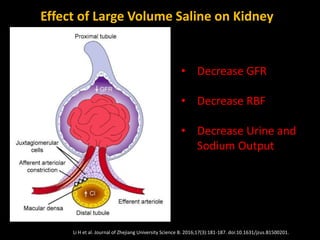
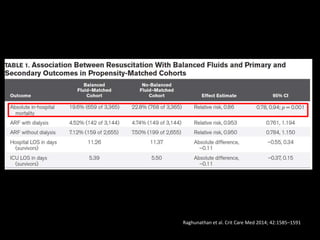
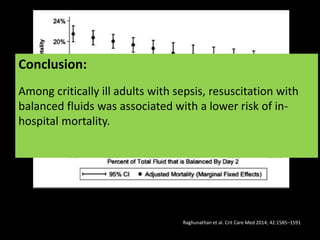
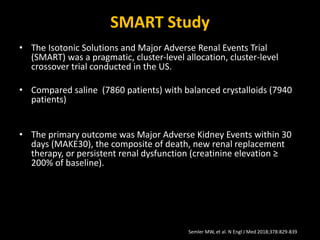
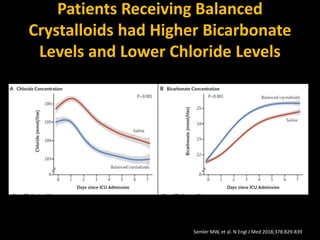
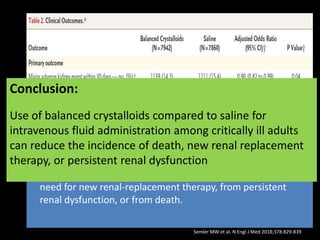
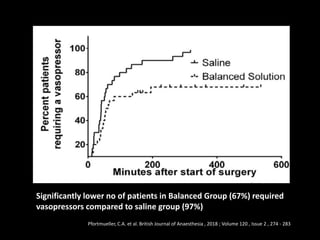
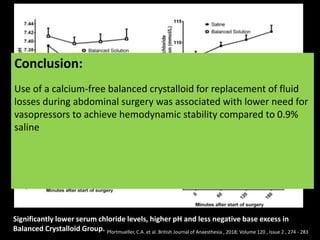
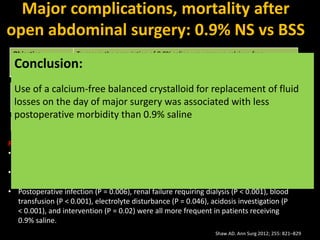
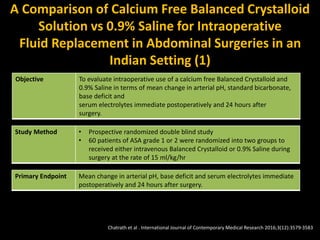
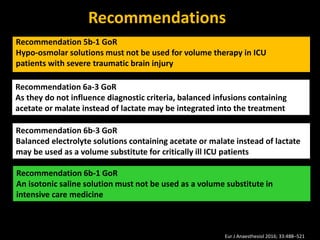
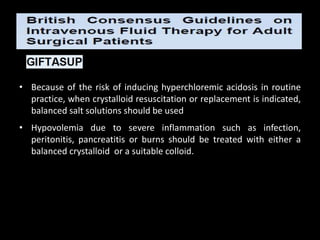
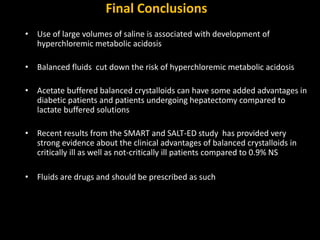
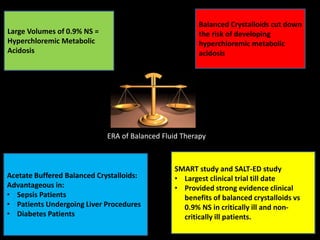
Balanced fluid therapy aims to strike the right balance in fluid choice and administration. While 0.9% saline was traditionally used, it is not physiologically balanced and can lead to issues like hyperchloremic acidosis. Balanced crystalloid solutions like Plasma-Lyte and Ringer's lactate better match the electrolyte composition of blood and have shown benefits over saline in clinical studies, with reduced complications and lower mortality in critically ill patients. Large trials like SMART and SALT-ED found balanced fluids reduced major kidney adverse events compared to saline without affecting other outcomes.
![Hyperchloremic Acidosis
• First described by Hartmann 1935
• Increased Cl- load increases dissociation of
water into H+ and OH-
• Acidosis is the result of an increase in [H+]
• Does this matter?](https://image.slidesharecdn.com/balancedfluidtherapy-drbchoudhuri-221117192558-164791ae/85/Balanced-Fluid-Therapy-Optimizing-Patient-Outcomes-in-Critical-Care-by-Dr-Bodhisatwa-Choudhuri-10-320.jpg)
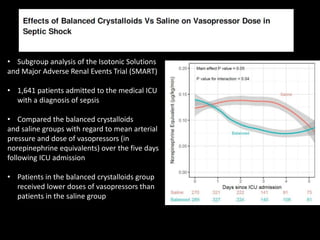

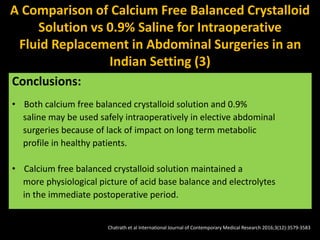
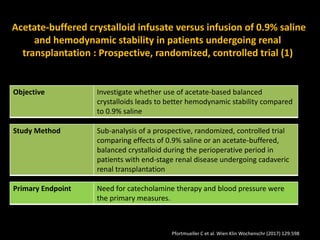
![Acetate-buffered crystalloid infusate versus infusion of 0.9%
saline and hemodynamic stability in patients undergoing renal
transplantation : Prospective, randomized, controlled trial (2)
Mean minimum arterial blood pressure was significantly lower in
patients randomized to 0.9% saline than in patients receiving the
balanced infusion solution (57.2 [SD 8.7] versus 60.3 [SD 10.2]
mm Hg, p = 0.024)
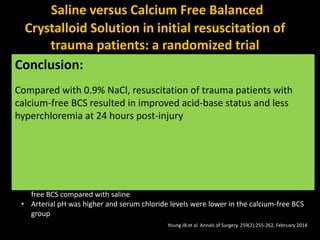
Conclusion:
• The use of an acetate-buffered, balanced infusion solution results
in reduced need for use of catecholamines and cumulative
catecholamine dose for hemodynamic support and in less
occurrence of arterial hypotension in the perioperative period.
• Further research in the field is strongly encouraged.
Pfortmueller C et al. Wien Klin Wochenschr (2017) 129:598](https://image.slidesharecdn.com/balancedfluidtherapy-drbchoudhuri-221117192558-164791ae/85/Balanced-Fluid-Therapy-Optimizing-Patient-Outcomes-in-Critical-Care-by-Dr-Bodhisatwa-Choudhuri-52-320.jpg)




























![Balanced Crystalloids Webinar February 2023[2207].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/balancedcrystalloidswebinarfebruary20232207-240501141244-58dce968-thumbnail.jpg?width=640&height=640&fit=bounds)

























































