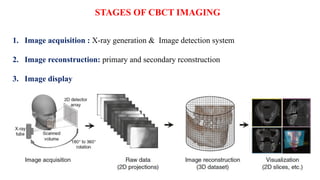
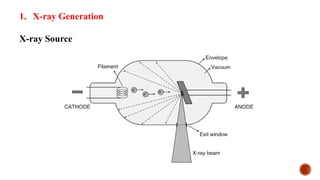
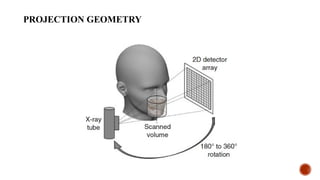
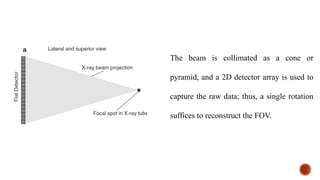
The document discusses Cone-Beam Computed Tomography (CBCT), detailing its principles, image acquisition, detection systems, and reconstruction processes. It highlights the technical elements required for optimal imaging, the various artifacts that can occur, and the advantages and disadvantages of using CBCT in dental radiology. Additionally, it emphasizes the importance of patient positioning and equipment preparation to improve imaging quality and minimize radiation exposure.