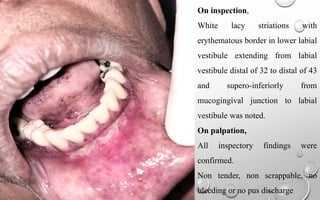
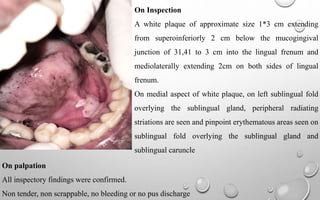
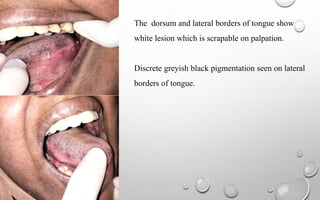
A 44-year-old female presented with a two-month history of burning sensation in the mouth and ulcerated mucosa, previously consulting a gastroenterologist and dental clinics without relief. Examination revealed erosive lichen planus and candidiasis with characteristic white lesions and erythematous borders on the lower labial vestibule and tongue. The treatment plan includes topical corticosteroids and oral medications, with follow-up scheduled.