This document provides an overview of the use of cone beam computed tomography (CBCT) in endodontics. It discusses the role of imaging in endodontics, compares 2D and 3D imaging, describes the principles and types of CBCT equipment, and reviews the clinical applications, advantages, limitations, and radiation dosage of CBCT. Key applications of CBCT in endodontics include evaluation of root canal anatomy, detection of apical periodontitis, assessment of root canal treatment outcomes, and pre-surgical planning.






![Assess the degree of curvatures
associated with the roots of teeth
Teeth with anatomical and
morphological anomalies such as dens
invaginatus and tooth fusion
In a study that evaluated 608 permanent mandibular second
molars using CBCT a higher prevalence of “C” shaped
canals was noticed [26,27]. CBCT is an effective tool for the
detection of additional distolingual roots and C-shaped
canals](https://image.slidesharecdn.com/cbctinendodonticsppt-200506025308/75/Cbct-in-endodontics-ppt-25-2048.jpg)




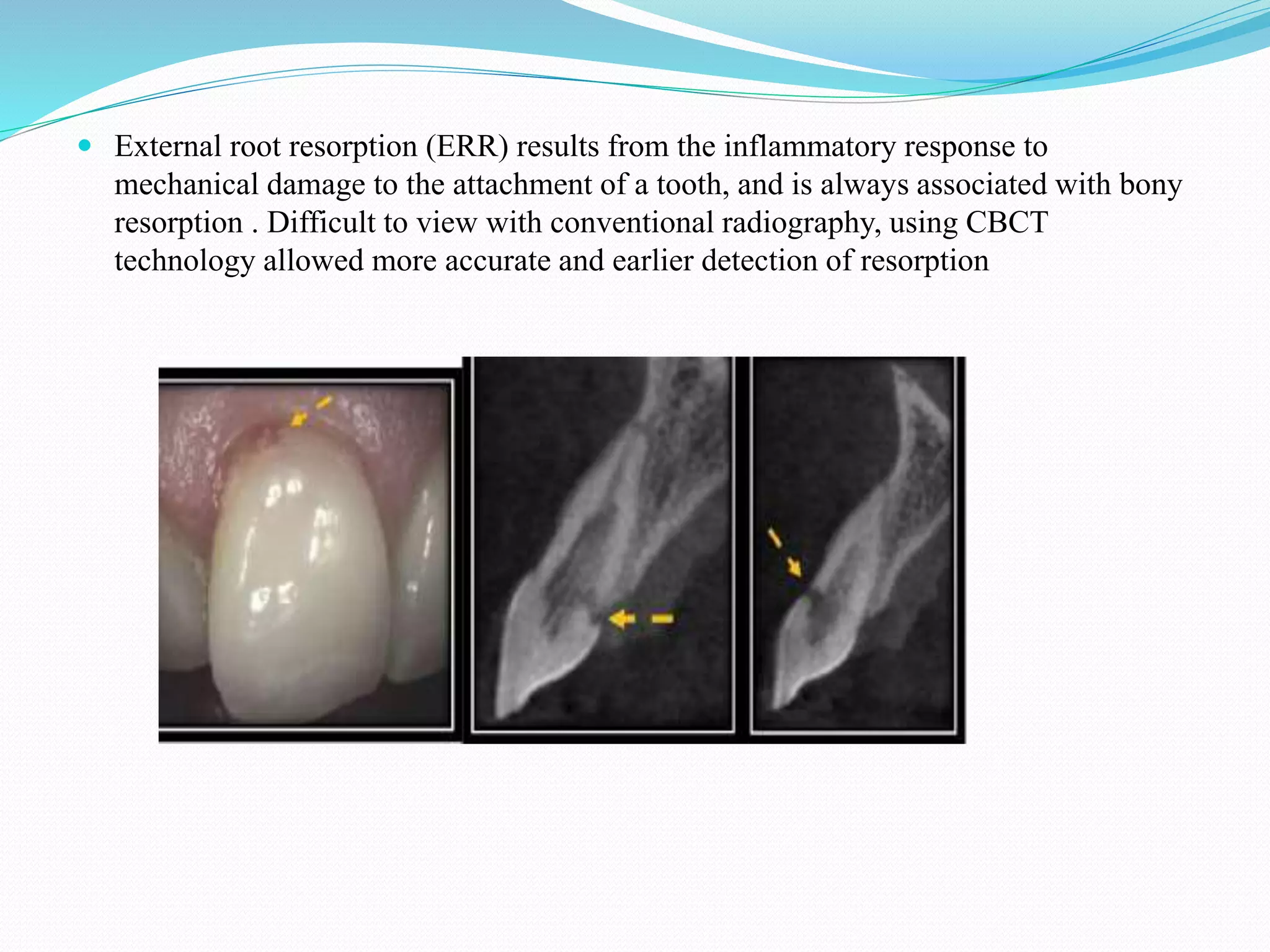
![ Root resorption is defined as the loss of dental hard tissues as a result of osteoclastic
activities. [58] It can be a physiological or a pathological phenomenon. The
diagnosis of root resorption is based primarily on radiographic examination, with
Internal root resorption (IRR) is a relatively rare occurrence, characterized by
structural changes of the tooth that appear as a widening of the root canal. IRR is
usually asymptomatic and is often detected on routine periapical and panoramic
radiographs (L. Levin and Trope, 2002; Patel and Dawood, 2007).](https://image.slidesharecdn.com/cbctinendodonticsppt-200506025308/75/Cbct-in-endodontics-ppt-36-2048.jpg)