




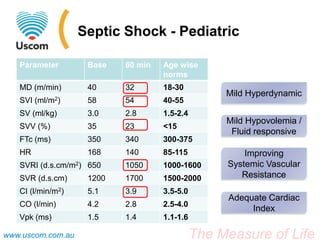





A 3-year-old boy with septic shock presented on the basis of persistent fever and respiratory distress, requiring transfer to the PICU where he underwent mechanical ventilation and treatment with fluid boluses and medications. His condition showed initial improvements but worsened after six hours necessitating additional interventions, including milrinone administration. The document outlines the dynamic nature of septic shock management and emphasizes the importance of monitoring hemodynamic changes for timely treatment decisions.

































































































