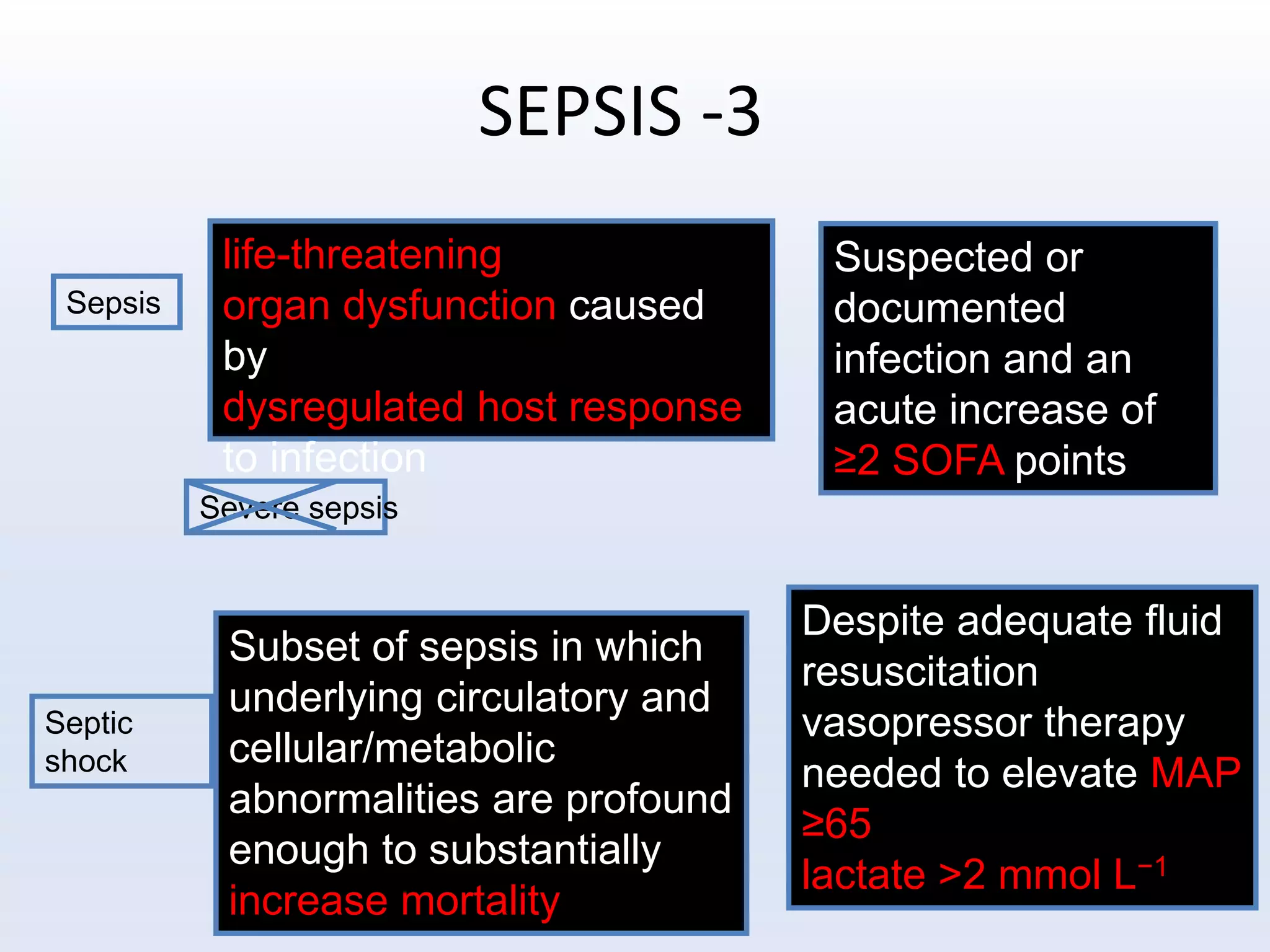
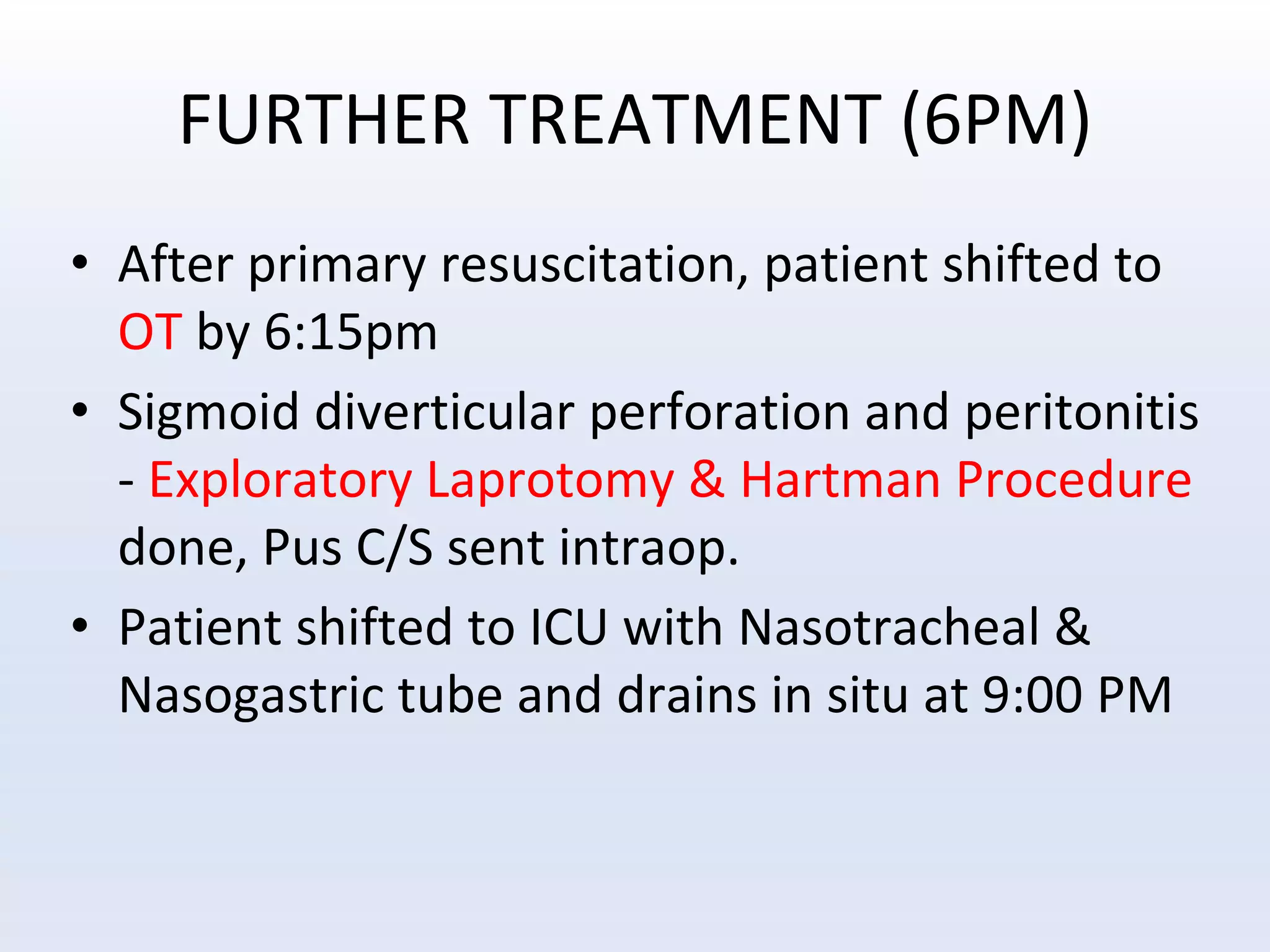
The document discusses a clinical case related to septic shock, covering definitions, management protocols, and treatment recommendations based on recent sepsis guidelines. It details the diagnosis, treatment procedures, and outcomes for a 64-year-old female patient with multiple health issues, ultimately leading to surgical intervention and post-operative care. The document emphasizes the importance of updated protocols in sepsis management to improve patient outcomes.