Download as PDF, PPTX
![• Usually over 50% of all new born infants become visibly
jaundiced because of,
High [Hb] at birth RBC breakdown
RBC life span of infants are short(70 days)
Less efficient bilirubin metabolism
Early neonatal jaundice is important :
# as it may be a sign of another disorder;
Eg: Haemolytic anaemia
Infection
Metabolic disease
Liver disease
# Unconjugated bilirubin deposition in basal ganglia may
cause Kernicterus](https://image.slidesharecdn.com/hashimpedscase-180828132933/85/case-presentation-on-neonatal-jaundice-27-320.jpg)
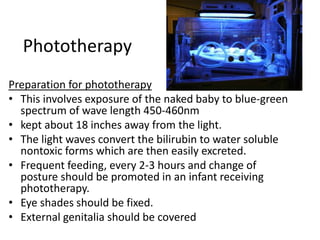

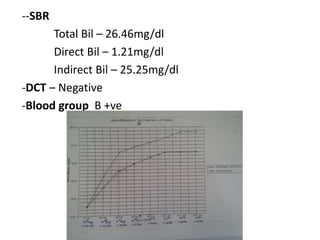
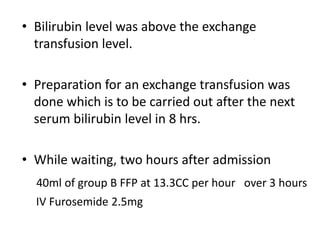
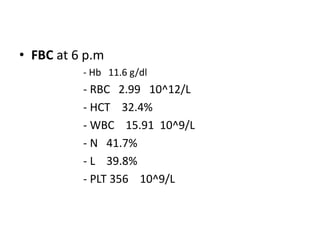
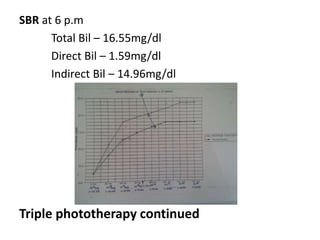
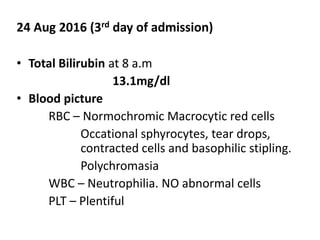
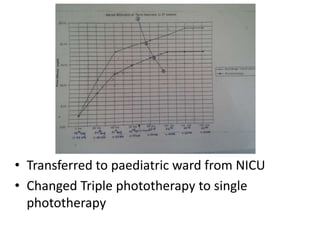
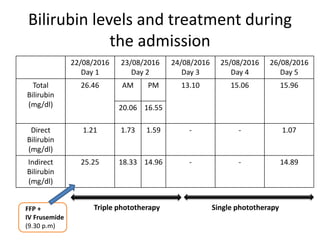
This case presentation describes a 3 day old baby boy who presented with jaundice. The baby's mother had borderline gestational diabetes that was controlled with diet. The baby was delivered via normal vaginal delivery at 37 weeks with good APGAR scores. On the third day of life, the baby developed yellowish discoloration of the skin and eyes. Initial workup found a serum bilirubin level above the exchange transfusion threshold. The baby was started on triple phototherapy and given IV fluids and FFP. Over the next few days, the bilirubin level decreased with phototherapy and the baby was discharged once the level was well below the phototherapy threshold.




































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
