Downloaded 104 times


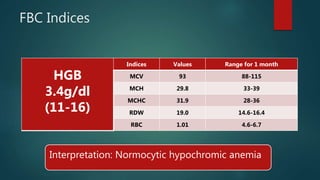
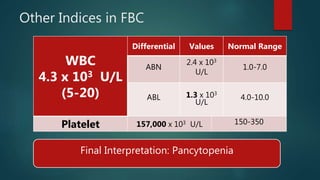
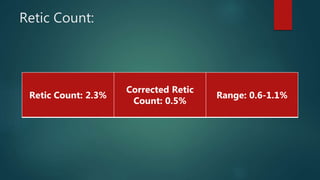


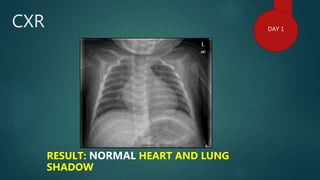
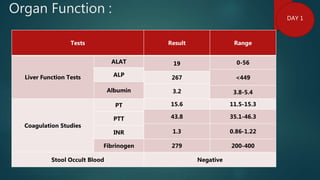
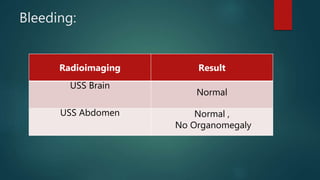
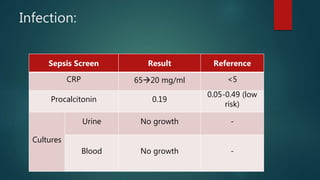
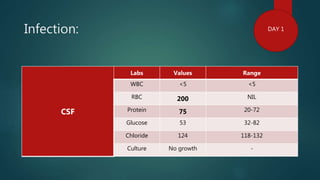
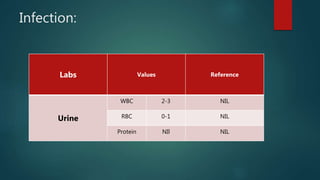
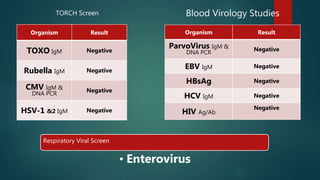
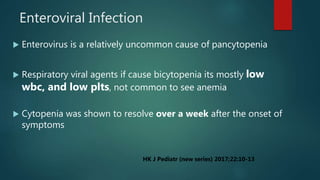
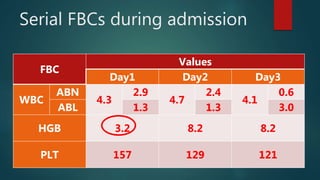
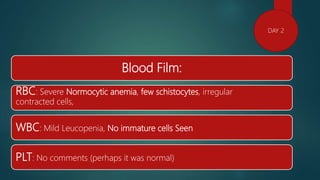
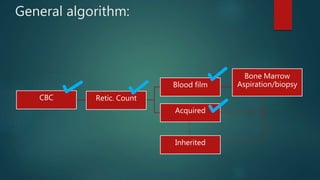
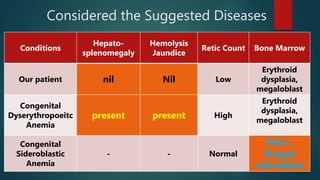


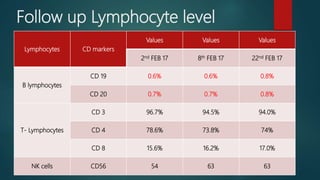
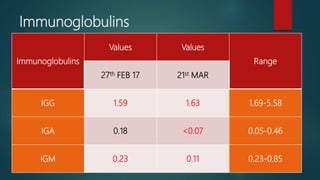
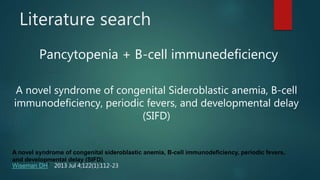

1. This case presents a 1.5 month old boy with pancytopenia, fever, and respiratory symptoms. 2. Initial workup showed normocytic anemia, leukopenia, thrombocytopenia, and low corrected reticulocyte count. Bone marrow aspiration found erythroid dysplasia and megaloblastic changes. 3. Further testing found B cell immune deficiency. The patient was eventually diagnosed with MYSM1 mutation, a rare cause of congenital sideroblastic anemia and immunodeficiency. He requires supportive care including transfusions and immunoglobulin therapy.







































































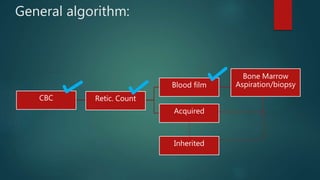
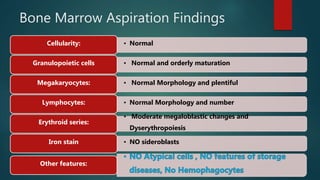
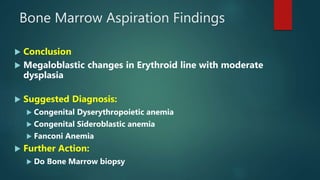
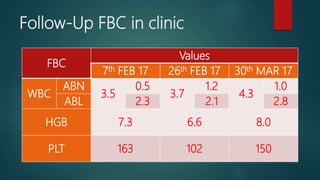
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















