Downloaded 15 times

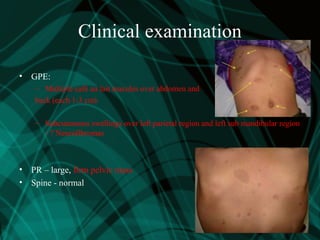
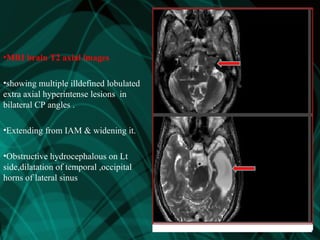
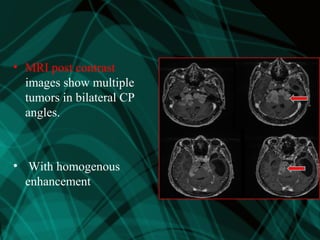
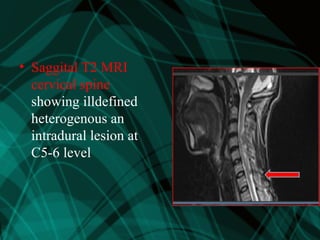
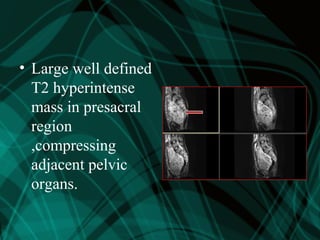
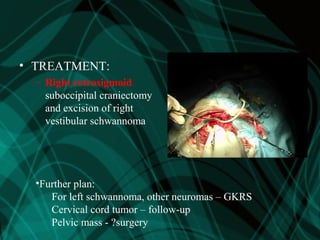
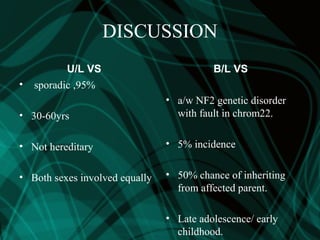



This patient presented with bilateral hearing loss, dizziness, and skin lesions. Imaging showed bilateral vestibular schwannomas, trigeminal schwannomas, a cervical tumor, and pelvic mass. The patient was diagnosed with neurofibromatosis type 2 (NF2) based on the multiple tumors. NF2 causes bilateral vestibular schwannomas and other tumors and has a genetic basis. The patient underwent surgery to remove the right vestibular schwannoma and will receive gamma knife radiosurgery for the remaining tumors. Early diagnosis and treatment of NF2 is important to prevent complete deafness and other complications.






























































































