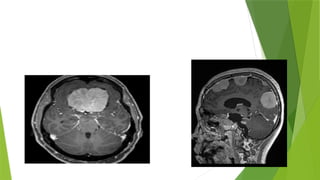
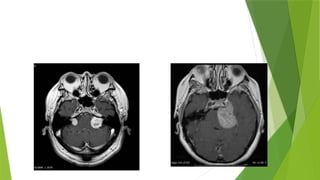
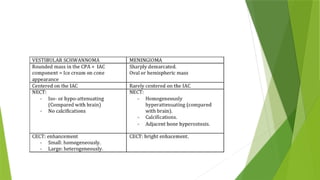
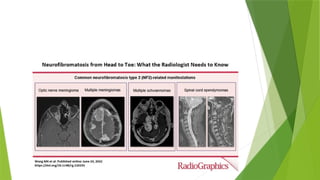
The document presents a case of a 22-year-old woman with eclampsia and vision loss, diagnosed with neurofibromatosis type 2 (NF2), characterized by multiple CNS tumors including schwannomas and ependymomas. MRI findings reveal significant mass lesions affecting the optic nerve, midbrain, and various brain regions, along with the presence of ependymoma lesions, which are typical of NF2. The document discusses the radiographic features, clinical presentations, and treatment options for schwannomas and ependymomas, highlighting their slow growth and potential for complete resection.




































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

