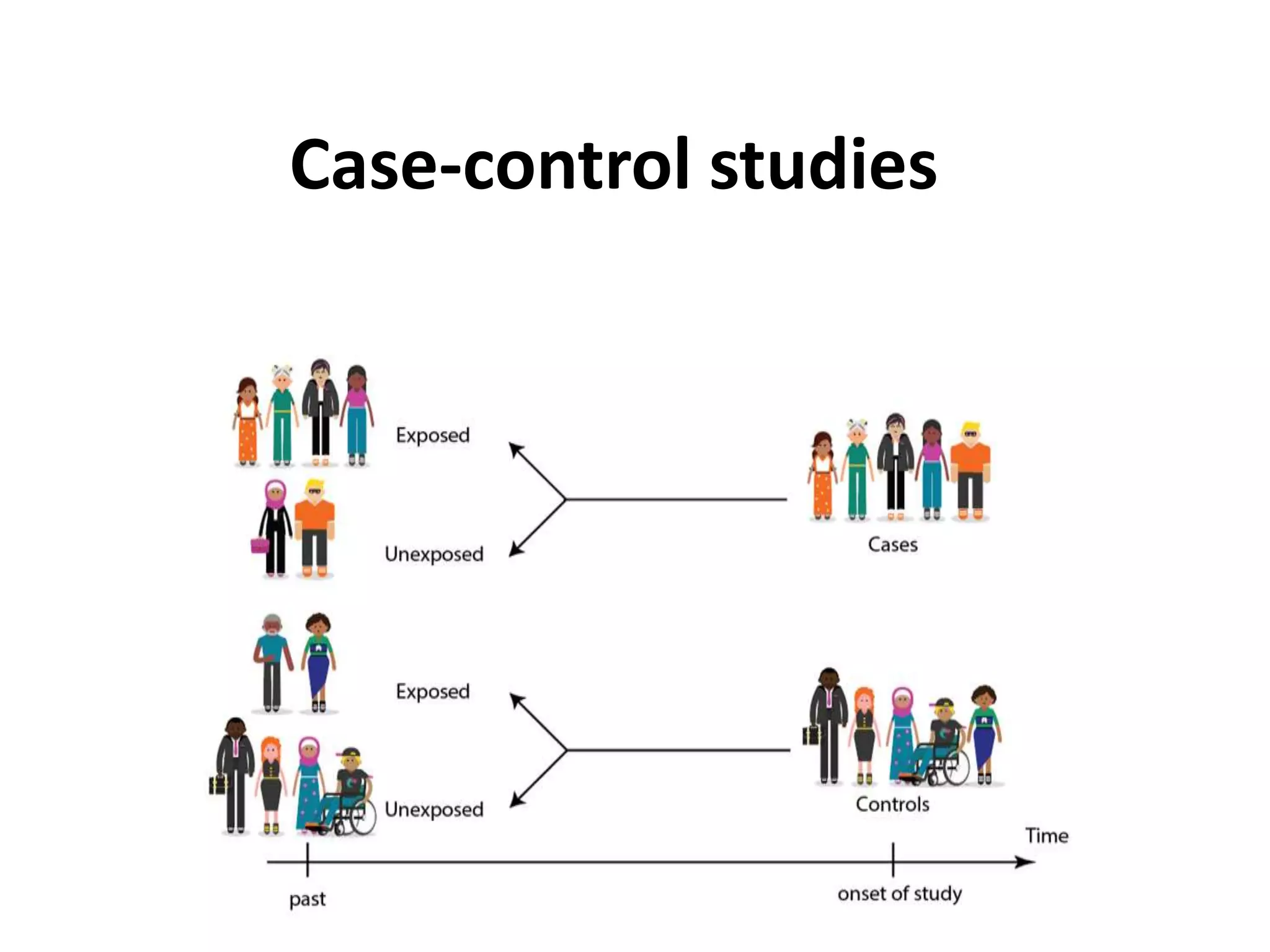












A case-control study compares exposures in individuals with an outcome of interest (cases) to those without the outcome (controls). Researchers recruit participants based on disease status and then collect exposure information. Case-control studies are observational, less expensive than cohort studies, and useful for rare outcomes. However, they can be prone to biases like selection and recall bias.






















































































