This document discusses cohort studies, including:
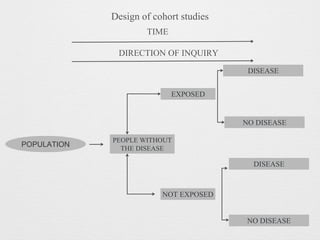
- Cohort studies follow groups of individuals over time to study how exposures affect disease outcomes.
- They can be prospective, following individuals not yet exposed, or retrospective, looking back at past exposure and disease data.
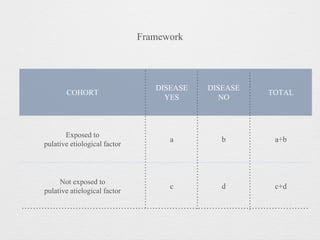
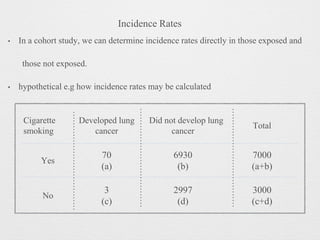
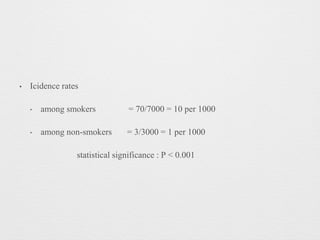
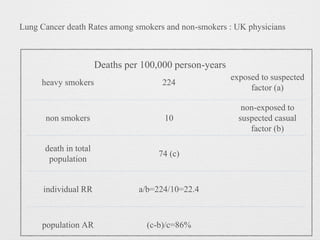
- Key elements include selecting study subjects, obtaining exposure data, selecting comparison groups, follow-up, and analysis of incidence rates and risk estimates like relative risk and attributable risk.
- Advantages are direct measurement of disease incidence and relative risks, while disadvantages include large sample sizes required.