Downloaded 65 times
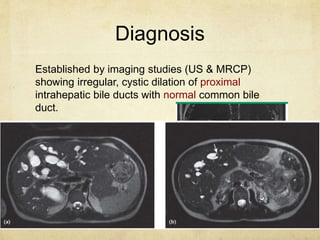

Caroli disease is a rare congenital condition characterized by saccular dilatation of the large intrahepatic bile ducts. It is caused by mutations in genes responsible for autosomal recessive polycystic kidney disease. Clinical manifestations vary depending on the age of onset and degree of hepatic or renal involvement, and can include biliary stones, bacterial cholangitis, and sepsis. Diagnosis is typically made through imaging studies showing cystic dilation of the proximal bile ducts. Treatment focuses on managing complications through supportive care or liver transplantation for recurrent cholangitis. Prognosis is variable depending on disease severity and any associated renal dysfunction.