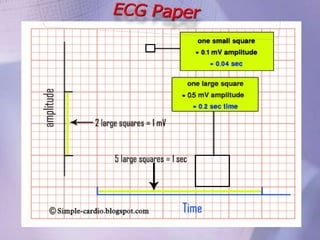
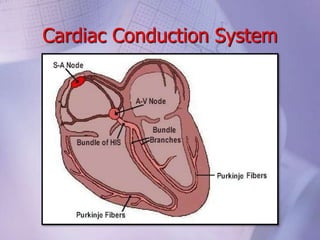
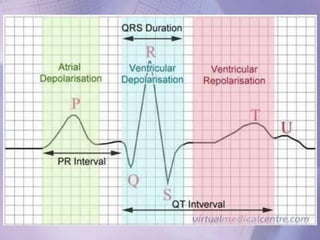
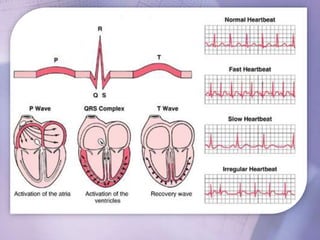
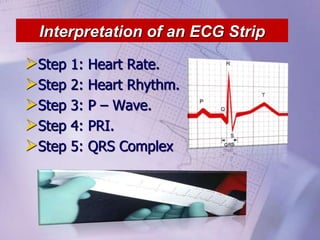
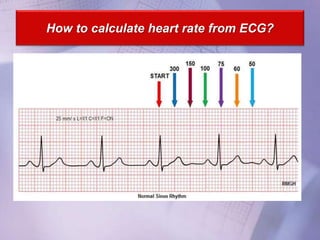
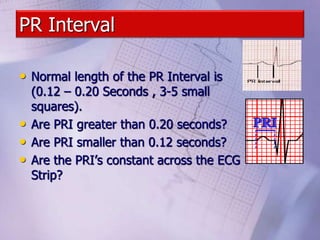
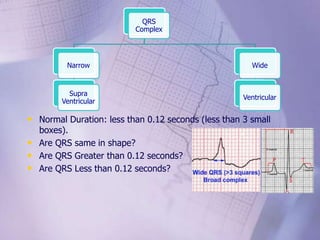
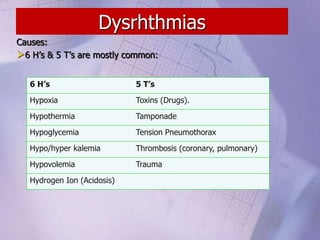
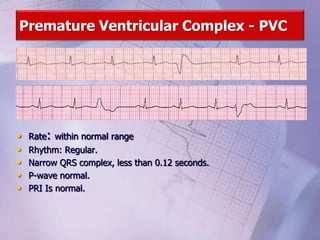
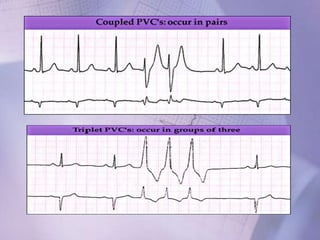
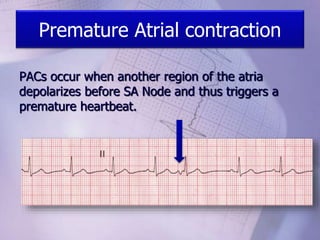

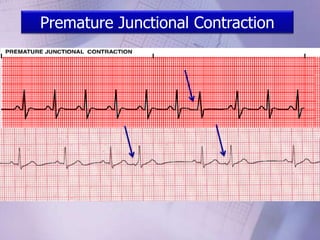
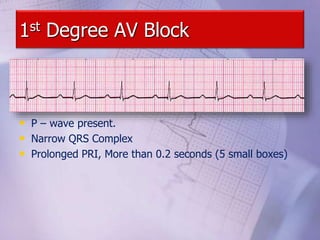

This document provides an overview of interpreting electrocardiogram (ECG) strips and identifying different cardiac rhythms and conduction abnormalities. It begins by outlining the key steps to interpret an ECG strip, including measuring heart rate, assessing rhythm, examining the P wave, PR interval, and QRS complex. Methods for calculating heart rate are described. Common rhythms such as normal sinus rhythm, bradycardia, junctional rhythms, premature ventricular contractions, atrial fibrillation, and ventricular tachycardia are defined. Various types of heart block and their characteristics are summarized. Causes and treatment options for different arrhythmias and clinical conditions are also reviewed.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








