Downloaded 70 times




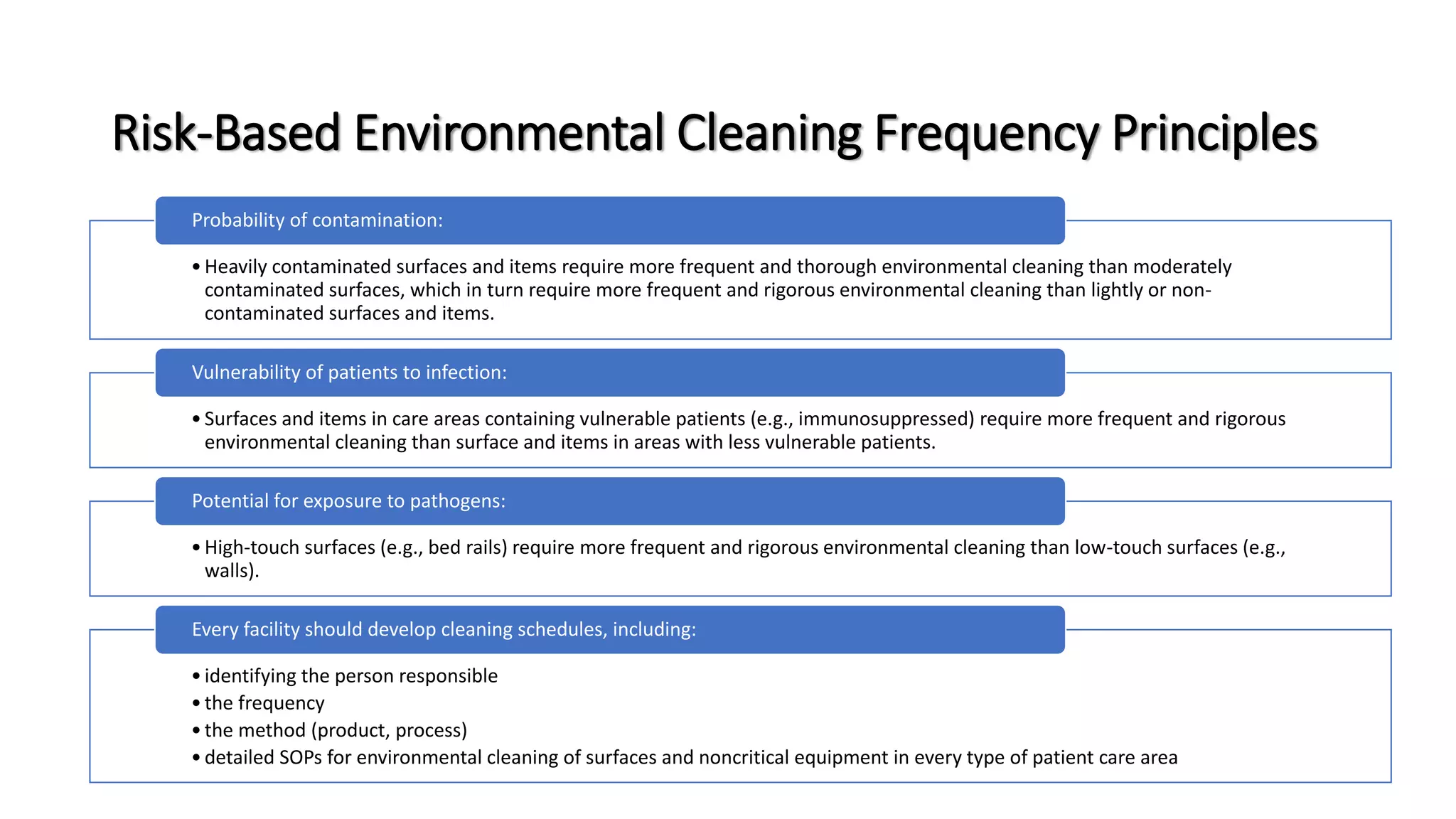
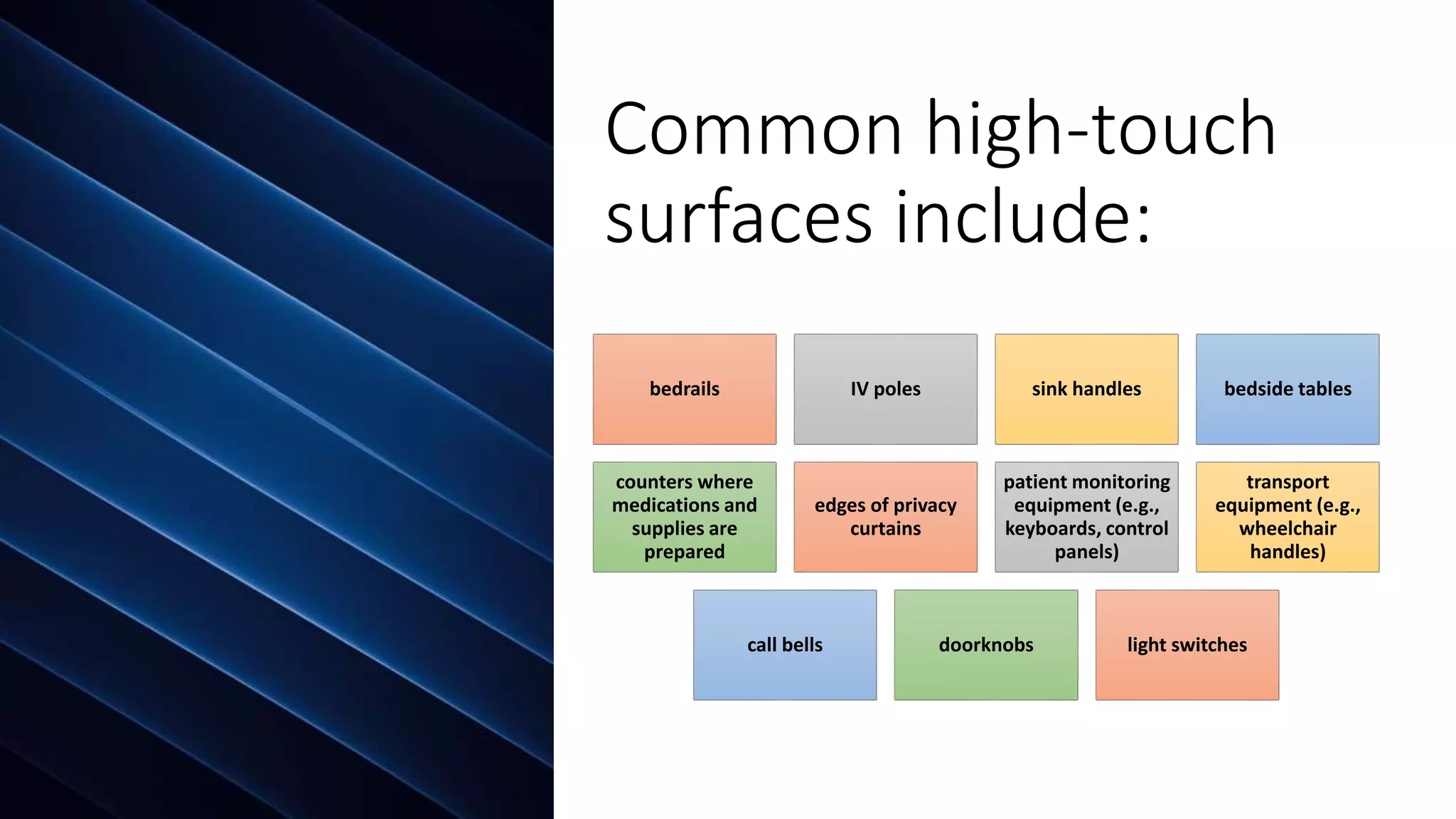

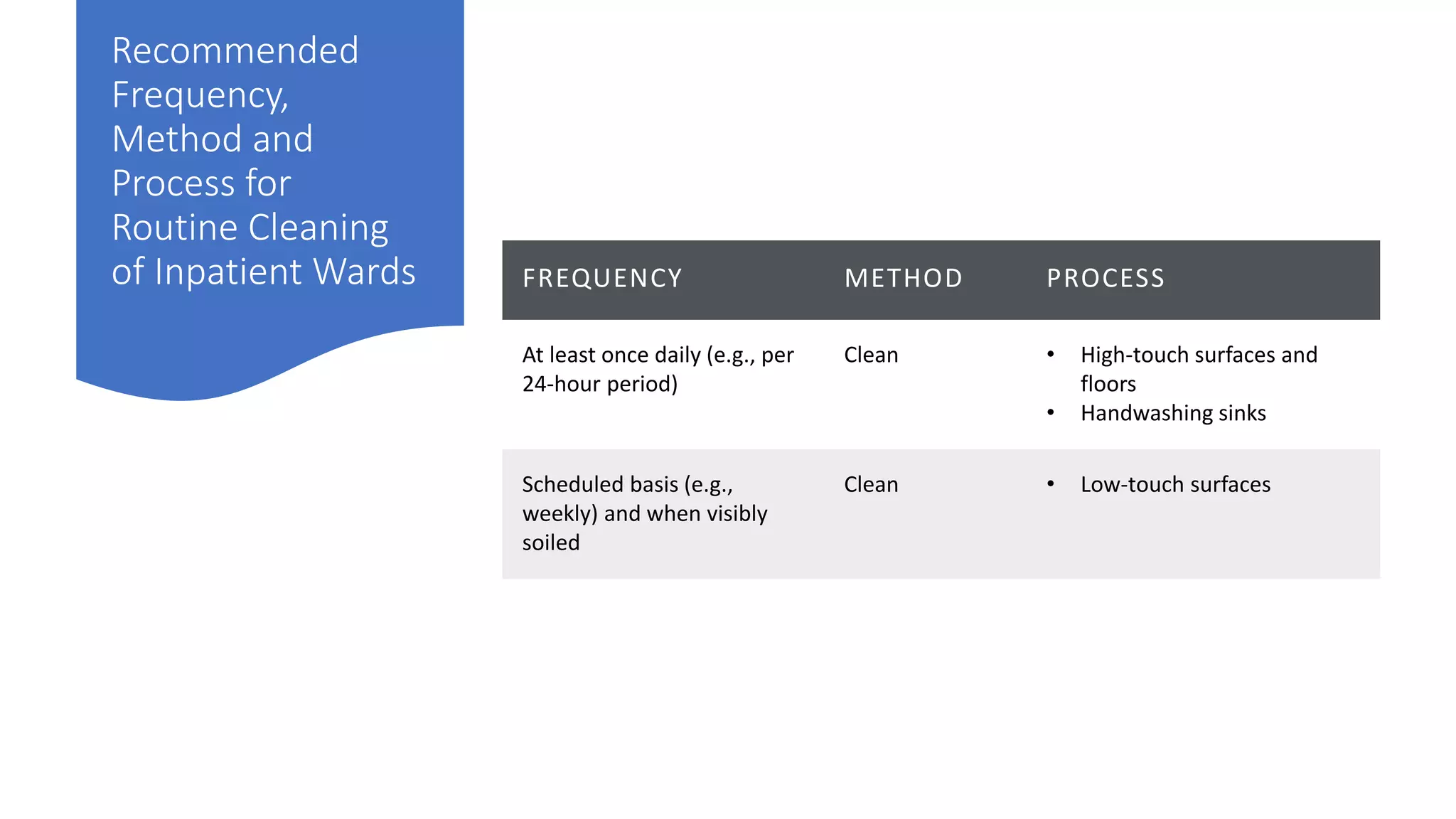

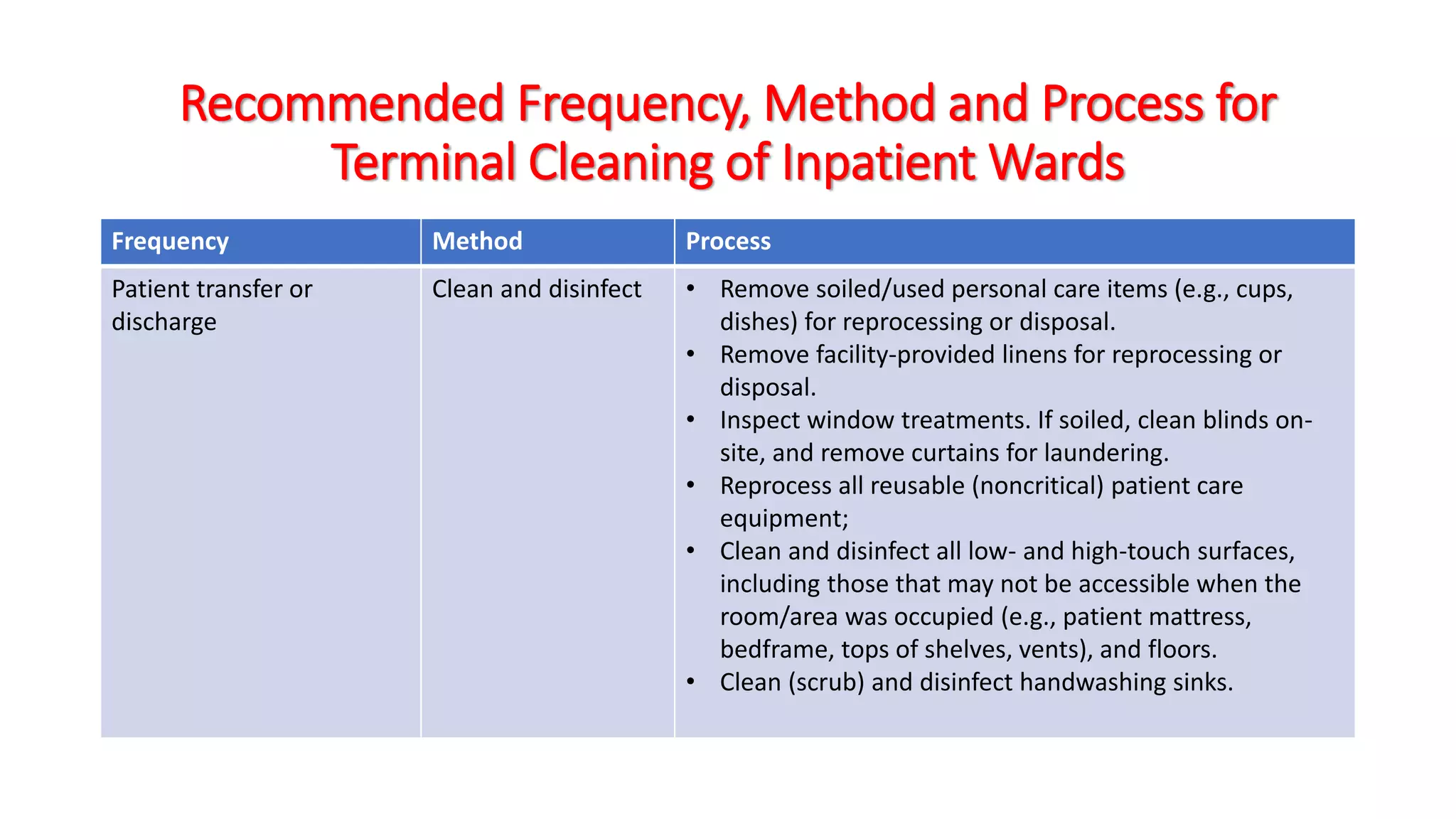

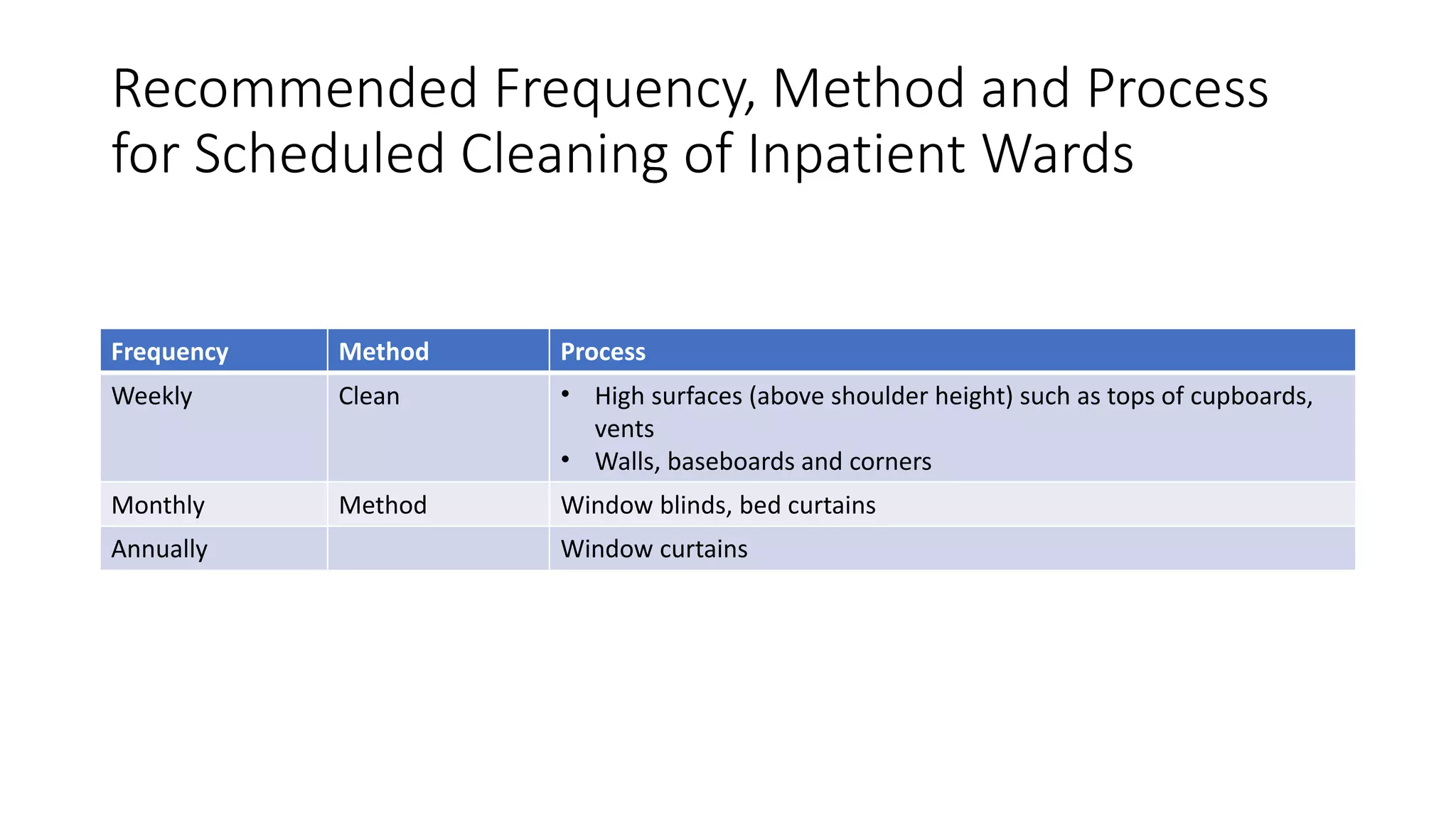






Cleaning and decontamination procedures in hospitals should be based on infection risk. This depends on likelihood of contamination, patient vulnerability, and surfaces' potential for exposure. There are three levels of decontamination: cleaning, disinfection, and sterilization. Cleaning removes organic matter but not necessarily pathogens. Disinfection reduces but may not kill all microorganisms. Different areas require different cleaning depending on activities. High-touch surfaces like bed rails require more frequent cleaning than low-touch surfaces.