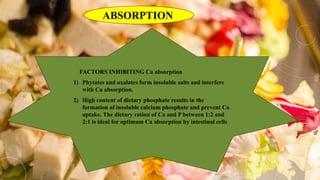
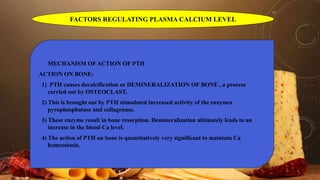
Calcium metabolism involves the distribution, daily requirements, dietary sources, functions, absorption, and factors regulating plasma calcium levels. Calcium is primarily stored in bones and teeth, with 99% located in the skeleton. Dietary sources of calcium include milk, dairy products, leafy greens, and fish. Calcium is important for bone formation, muscle contraction, blood coagulation, and enzyme activation. Absorption occurs primarily in the small intestine and is influenced by vitamin D, PTH, pH, and dietary factors like oxalates. Plasma calcium levels are tightly regulated by vitamin D, PTH, and calcitonin. Disorders of calcium metabolism include hypercalcemia, hypocalcemia, rickets, and oste






















































![REFERENCES
• Satyanarayana.U, Chakrapani.U, Essentials Of Biochemistry , Second
Edition; 2007.
• Burket LW, Greenberg MS, Glick M. Burkets oral medicine: diagnosis &
treatment. Hamilton, Ont.: BC Decker; Eighth edition ,2003.
• Sanjeev Mittal, Deepak Gupta1, Sahil Sekhri, Shivali Goyal Oral Manifestations of
Parathyroid Disorders and Its Dental Management, Journal of Dental and Allied
Sciences ¦ Jan-Jun 2014 ¦ Volume 3 ¦ Issue 1
• Andréia Pereira SOUZA, Tatiana Yuriko KOBAYASHI, [...], and Thais
Marchini OLIVEIRA, Dental manifestations of patient with Vitamin D-resistant
rickets, J Appl Oral Sci.2013 Nov-Dec; 21(6): 601-606](https://image.slidesharecdn.com/calmetabolism-200618183307/85/Cal-metabolism-62-320.jpg)