Download to read offline



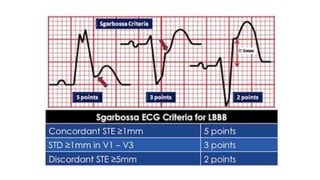
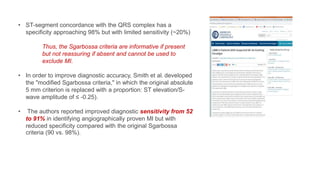
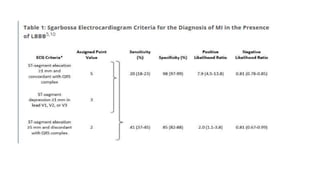


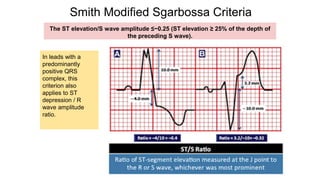




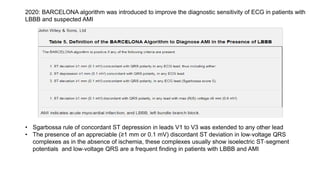
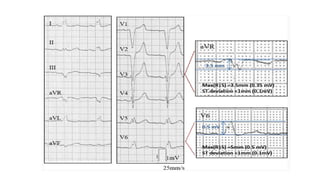

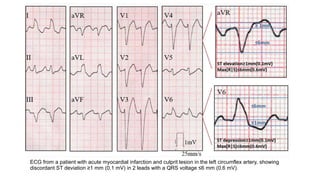

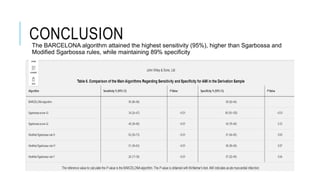


This document discusses left bundle branch block (LBBB) in the context of acute myocardial infarction (AMI). It provides an overview of LBBB and challenges in diagnosing AMI when LBBB is present. Several criteria are discussed for identifying AMI in the setting of LBBB, including the original Sgarbossa criteria from 1996, modified Sgarbossa criteria from 2012, and the Barcelona algorithm from 2020. The Barcelona algorithm achieved the highest sensitivity while maintaining good specificity for diagnosing AMI when LBBB is present. An ECG example is also provided to demonstrate positive Sgarbossa criteria.



































































