Downloaded 22 times



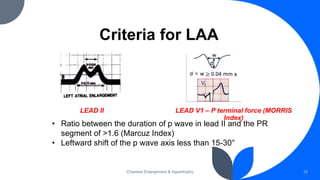
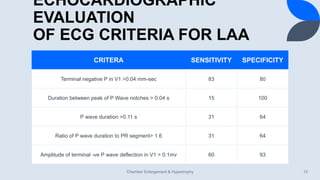
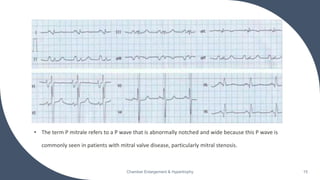
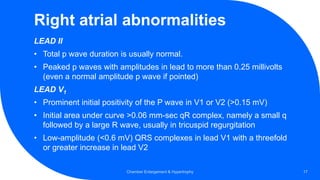
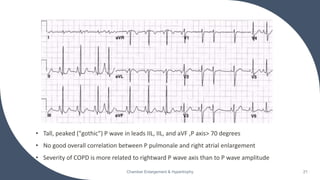
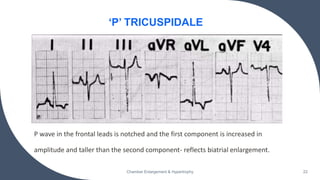
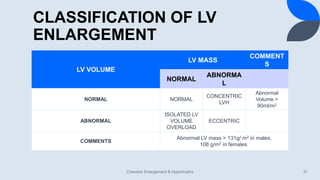
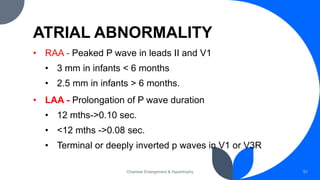
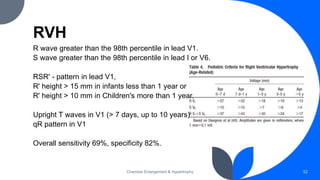
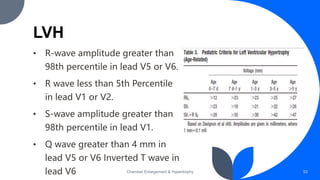

The document discusses the role of ECG in detecting cardiac chamber enlargement. Some key points: - ECG can detect chamber enlargement through changes in waveform morphology, amplitude/voltage, axis, and duration. These changes apply to both P waves and QRS complexes. - Common ECG criteria for left atrial enlargement include prolonged/notched P waves in lead II and terminal negative deflection in lead V1. For right atrial enlargement, criteria include tall peaked P waves in leads I, II, III and V1. - Common ECG patterns of left ventricular hypertrophy include tall R waves in left chest leads, ST-T wave changes, and prolonged QRS duration













































































