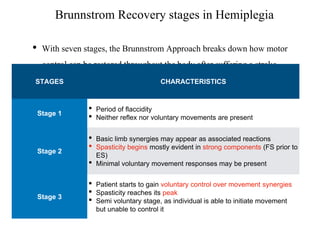
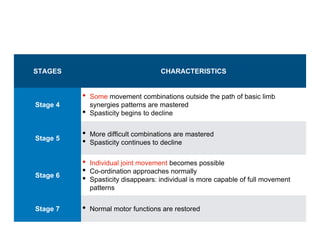
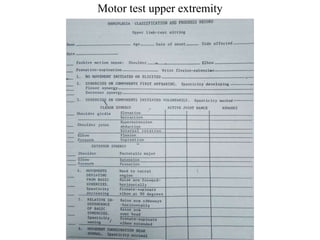
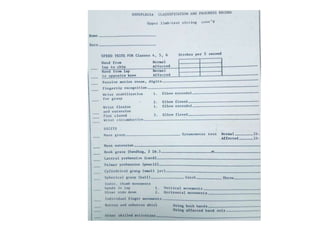
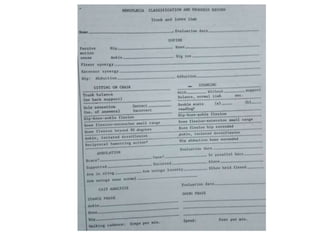
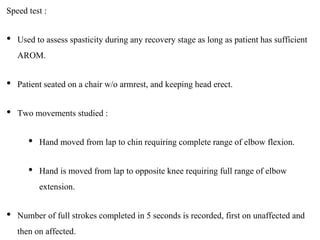
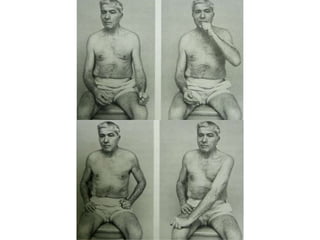
The Brunnstrom Approach is a neurodevelopmental treatment approach for stroke rehabilitation developed in the 1970s. It involves 6 stages of motor recovery: 1) flaccidity, 2) appearance of spastic synergies, 3) semi-voluntary movement, 4) combining movements, 5) complex voluntary movement, 6) restoration of normal movement. Treatment progresses the patient through these stages using reflexes, associated reactions, proprioceptive stimuli and resistance training. Evaluation assesses motor function, sensory loss, and spasticity through tests of range of motion, grasp, and speed of movement. The goal is to facilitate normal motor control and functional use of the affected limb.