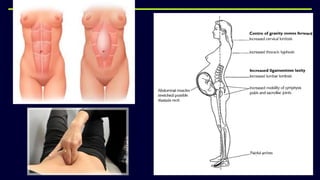
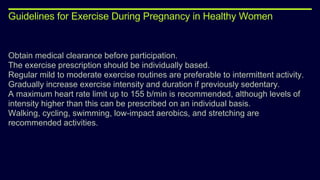
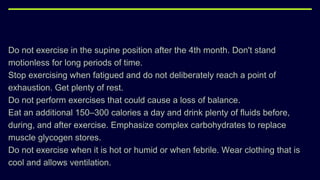
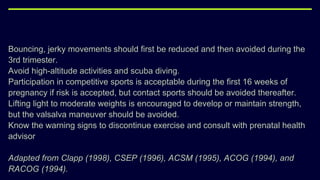
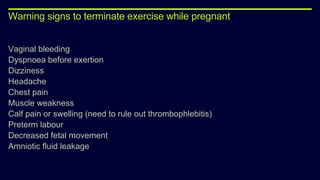
This document provides an overview of physical and physiological changes during pregnancy and guidelines for exercise during pregnancy and the postnatal period. It discusses the structural, metabolic, and physiological changes that occur in each trimester of pregnancy, as well as contraindications and benefits of antenatal and postnatal exercises. The document also reviews evidence from studies on the effects of aerobic exercise, pelvic floor exercises, acupuncture, and other physiotherapy modalities in treating pain and other issues during pregnancy and the postnatal period.










![PT management in CKD [Renal Rehabilitation].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptmanagementinckdrenalrehabilitation-220727071020-ee721238-thumbnail.jpg?width=640&height=640&fit=bounds)








































![4 - Anten';l';l';l';\][]\[\][\][\][]\atal care.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/4-antenatalcare-240319125644-b7d1db1e-thumbnail.jpg?width=640&height=640&fit=bounds)




















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









