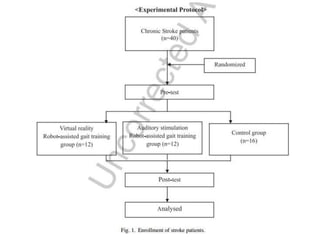
The document presents a study on the effects of robot-assisted gait training with virtual reality and auditory stimulation on balance and gait abilities in stroke patients. It details the methodologies, outcomes, and significant improvements observed in the experimental group compared to conventional therapy. The study concluded that robot-assisted interventions enhance functional activity and balance in stroke patients, though it has limitations regarding generalizability and duration.