Downloaded 1,411 times






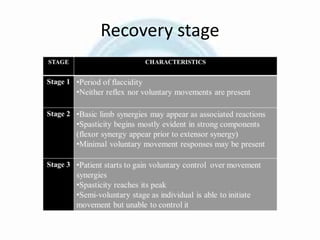
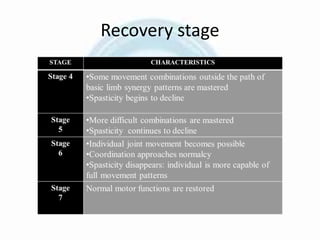

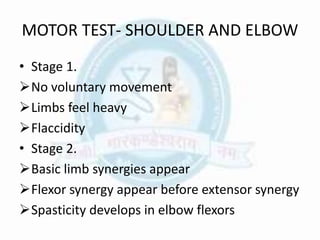
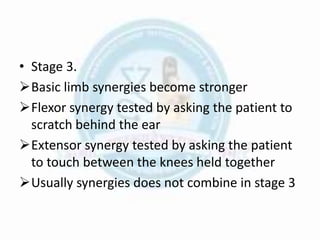
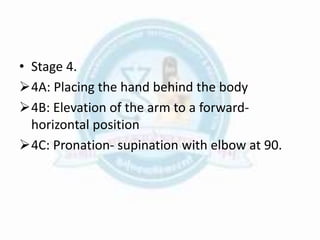

The Brunnstrom concept is a theoretical model of motor recovery following central nervous system injury developed by physical therapist Signe Brunnstrom. It is based on the hierarchical reflex theory and assumes that lower level reflexes get incorporated into purposeful movements through higher centers. Recovery proceeds from primitive reflexive movement to voluntary isolated movements. Treatment involves facilitating this progression using reflexes, associated reactions, proprioceptive and exteroceptive stimuli, and resistance. Motor and sensory function is evaluated using Brunnstrom's staging which characterizes recovery in a sequential progression.














































































