Downloaded 490 times
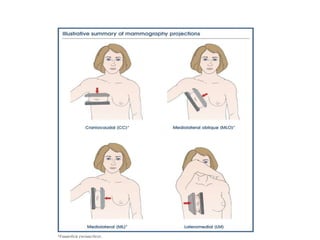
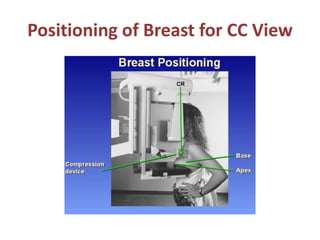
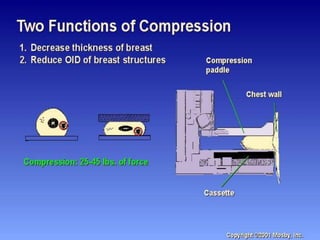
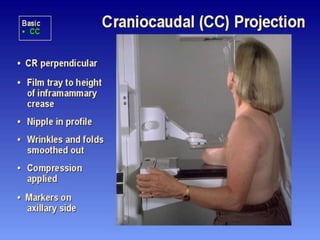
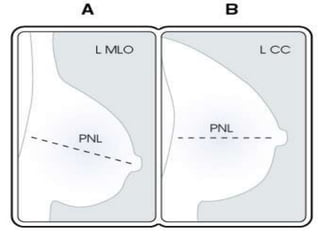
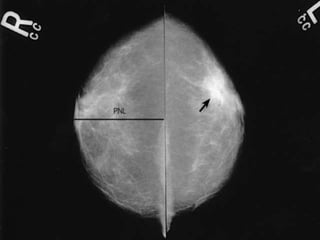
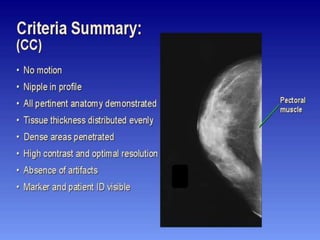
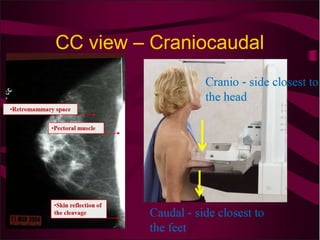
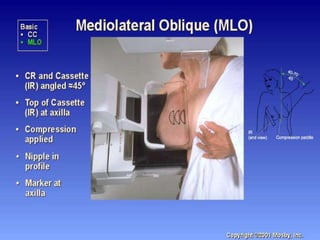
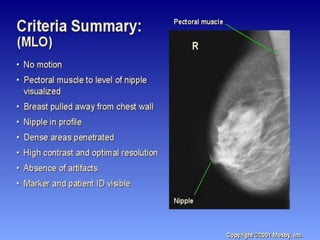
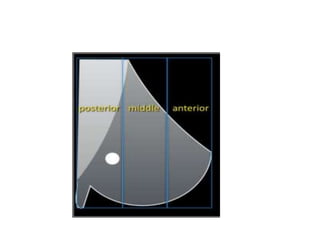
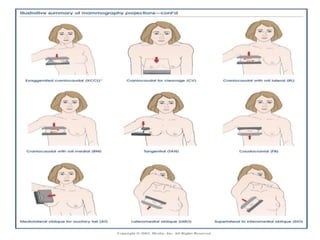
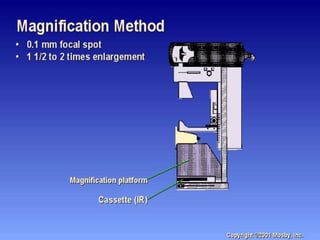
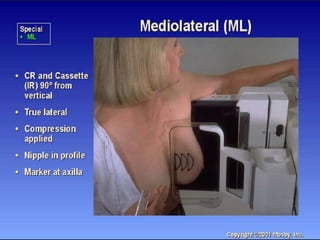
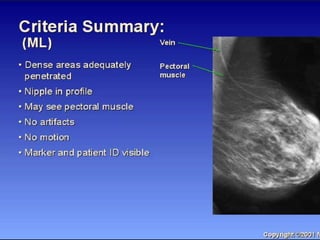


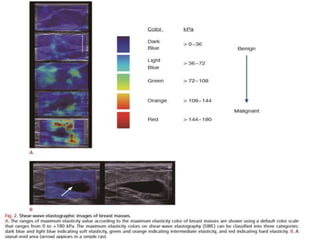





This document provides an overview of various breast imaging modalities including mammography, galactography/ductography, stereotactic guided procedures, digital tomosynthesis, ultrasound elastography, and MRI of the breast. Key imaging techniques are described such as mammography positioning, ductography technique, stereotactic biopsy procedures, and interpretation of ultrasound elastography images. Evaluation of breast lesions and interpretation of different imaging findings are also discussed.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




