Downloaded 30 times

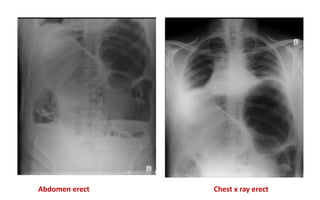
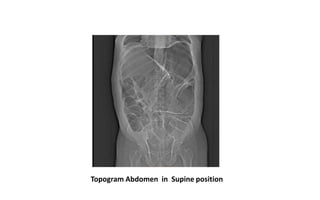
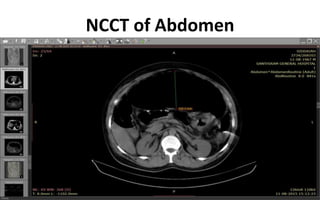







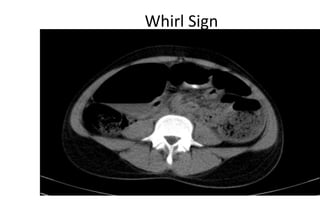



A 48-year-old male presented with abdominal pain and distension for 5 days. Imaging revealed transverse colon volvulus, which was confirmed during surgery. Transverse colon volvulus is rare, accounting for only 2-4% of intestinal obstructions. It carries a higher mortality risk of 33% compared to 21% for sigmoid volvulus and 10% for cecal volvulus. Surgical detorsion and resection of the affected colon segment is usually required to prevent recurrence.



















































































