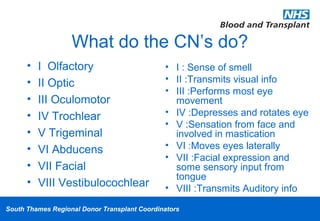
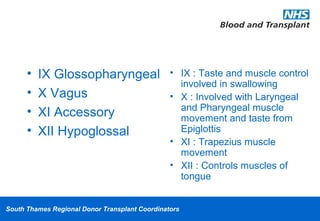
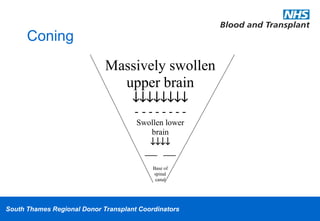
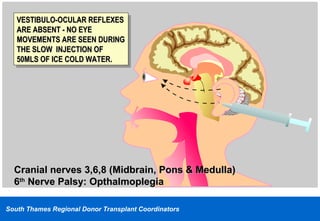
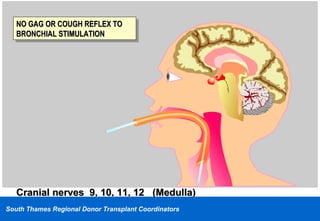
This document discusses brain stem death testing and organ donation. It begins by defining brain stem death as the irreversible loss of consciousness and breathing capacity. It then describes how brain stem death is diagnosed by testing the function of 12 cranial nerves and observing the lack of respiratory effort during an apnea test. The document outlines the signs and causes of brain stem injury and death, as well as the importance of optimizing organ donor physiology after death is declared to facilitate transplantation.