CONTENTS
• INTRODUCTION
• HISTORY
•DEFINITION
• APPROACH TO THE CLINICAL DIAGNOSIS OF BRAIN
DEATH
• DOCUMENTATION AND CERTIFICATION
• PATHOPHYSIOLOGICAL CHANGES AFTER BRAIN
DEATH
3.
INTRODUCTION
• Preceding 1950s,the concept of death revolved around
cessation of cardio-respiratory function .
• Development of advanced life support measures including
cardiopulmonary resuscitation and positive pressure ventilation
brought this interdependence and the traditional definition of
death into question .
4.
HISTORY
• 1959 –first described in the French & Scandinavian literature
proposing a name for the death of the nervous system- le coma
depasse by MOLLARET AND GOULON.
• 1968 – the concept of the brain death as death and the clinical
and EEG criteria was proposed by an Ad hoc committee of
Harvard medical school.
• 1976 – UK Royal medical college defined brain death as complete
irreversible loss of brainstem function and specified clinical
criteria to certify brain death.
5.
• 2023 –after revision of 2010, 2011 AAN /AAP/CNS/SCCM
PEDIATRIC & ADULT BRAIN DEATH–Consensus Practice
Guidelines
6.
DEFINITION
• Brain deathis defined as a permanent cessation of all functions
of the brain in which the individual organs may function but
lack integrating function of the brain, lack respiratory drive ,
consciousness and cognition.
• The three essential findings in brain death are coma, absence
of brainstem reflexes, and apnoea.
• Brain death is a clinical diagnosis.
8.
APPROACH TO THECLINICAL DIAGNOSIS OF
BRAIN DEATH
• Identification
• Formal clinical testing
• Ancillary tests of brain death
• Declaration of death
• Who should do the tests?
• Communication, organ donation and other considerations.
9.
IDENTIFICATION
• Patients inICU with poor GCS.
• Proof that the clinical condition is due to irreversible structural
brain damage-
o Traumatic brain injury
o CVA –ischaemic or hemorrhagic
o Hypoxia or metabolic insult to neuronal tissue
• Exclusion of reversible causes of coma
10.
PREREQUISITES FOR CLINICALTESTING:
• Absence of hemodynamic shock
• Established etiology and absence of reversible etiologies to
explain the coma
• Competency of the health care professional performing the
clinical determination
• Competency of the health care professional performing and
interpreting ancillary laboratory testing
11.
CONFOUNDING CONDITIONS
• Hypothermia
•(CNS) depressing drugs that may explain or contribute to coma (iv
sedatives-dexmedetomidine, etomidate , ketamine, midazolam
propofol; antiseizure drugs–clonazepam , diazepam,
levetiracetam, lorazepam, barbiturates ,valproate ,phenytoin).
• High cervical spine injury
• Evidence of acquired or iatrogenic neuromuscular paralysis, e.g.,
Guillain-Barré syndrome, Residual neuromuscular blockade
• Severe acid-base, electrolyte, endocrine abnormality that may
explain or contribute to coma Shock
12.
• In caseof hypoxia or cardiac arrest wait for 24 hrs following
the episode inorder to diagnose brain death.
• In case of any suspected drug intoxication (sedative ,toxin,
neuromuscular blocking agents) -wait for atleast 5 half lives
where the drug can be eliminated.
• In renal or hepatic failure ,hypothermia –time lapse before
diagnosing brain death is around 50-100 hours
13.
BRAIN DEATH DIAGNOSIS
•Exclude the reversible causes of coma
• Determine the cause of coma
• Establish irreversibility
15.
• Hypothermia suppressesCNS function → misdiagnosis of brain
death
• Body temperature must be within normal range (i.e.,
hypothermia must be corrected) before the criteria for brain
death are applied.
• Hypotension may result in compromised cerebral perfusion
leading to loss of electroencephalographic activity, thus causing
a spurious diagnosis.
16.
•METABOLIC
Ammonia >75 micromol/L
BUN>75mg /dl
Calcium <7mg or >11mg/dl
Glucose <70mg/dl or > 300mg/dl
Magnesium <1.5 mg/dl or > 4mg/ dl
Potassium <3mmol/L or > 6 mmol /L
Sodium <130mmol/L or >160 mmol/L
•ACID-BASE
pH <7.3 or >7.5
TO ESTABLISH THECAUSE OF COMA
• Coma with GCS of 3 owing to irreversible acute brain
damage of known etiology
• History of traumatic anoxic or metabolic brain injury
Progression of injury over time that can explain events
• Affect both hemispheres and brainstem.
• To have clear and definite clinical and/or neuroimaging
evidence of an acute central nervous system (CNS) insult
that is consistent with the irreversible loss of neurological
function
19.
IRREVERSIBILITY
• Irreversibility meansthat no treatment may be reasonably
expected to change the condition.
• Irreversibility usually rely on repeated assessment over time.
• A repeat clinical evaluation and documentation 6 hours later
is advised, but this time is variable
21.
DIAGNOSTIC CRITERIA
• Brainstem death is a clinical diagnosis in most countries.
• Clinical tests = accurate, reliable, reproducible and easy to
carry out
• Neurological examination consists of 3 steps:
– Documentation of Deep unresponsive coma
– Documentation of Absent brain stem reflexes
– Documentation of Absent respiratory efforts confirmed by
apnoea test
22.
Documentation of DEEPUNRESPONSIVE COMA
• COMA: complete loss of consciousness, vocalization and
volitional activity.
• A comatose patient shows absence of responsiveness to
all noxious stimulation including auditory , visual and
tactile stimulation.
• Spinal reflexes or motor responses, confined to spinal
distribution may be present in brain dead patients.
23.
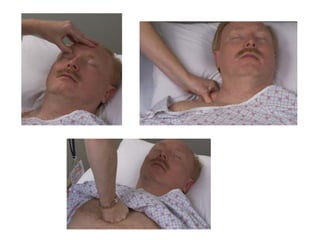
MOTOR RESPONSE TOPAINFUL STIMULI
• CENTRAL PAINFUL STIMULI can be given in the form of supra
orbital pressure, trapezius squeeze and sternal pressure
• Thumb pressure over the supra orbital groove (trigeminal
nerve sensation) or deep pressures on condyles of TM joint
• Response : Grimacing (facial nerve motor response)
• CNS-mediated motor response to pain in any other
distribution, seizures, and decorticate and decerebrate
responses impede BD diagnosis
25.
LAZARUS SIGN
• Motorresponses may occur spontaneously during apnea testing,
often during the hypoxic or hypotensive episodes.
• They include spontaneous movements of limbs other than
pathologic flexion or extension response and respiratory like
‑
movements (shoulder elevation and adduction, back arching,
intercostal expansion without significant tidal volumes) and
should not be misinterpreted as evidence of brain stem function.
• Patient briefly raises arms and drops them across their chest
and this response is of spinal origin.
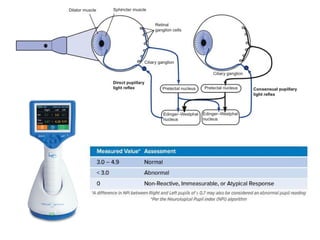
PUPILLARY REFLEX: Pupillaryresponse to light
• direct and consensual, is considered one of the most
discriminant reflexes in BD diagnosis.
• Both widely dilated as well as mid positioned fixed pupils are
‑
seen in brain dead patients.
• The size may vary from 4 9 mm.
‑
• Dilated pupils are compatible with brain death because
sympathetic cervical pathways connected with the radially
arranged fibres of the dilator muscle may remain intact
30.
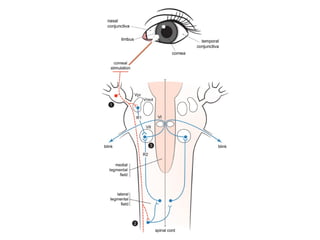
CORNEAL REFLEX
• Unilateralcorneal stimulation with a throat swab induces a
bilateral closure of the eyelids.
• A bilateral or unilateral response of eyelid closure and upward
deviation of the eye (Bell’s phenomenon) indicates preserved
brainstem functioning.
• However, oedema or drying of the cornea, and severe facial
and ocular trauma may preclude a satisfactory stimulus for this
reflex.
• Moreover, the threshold for excitation decreases markedly if
the lids are kept closed
32.
OCULOCEPHALIC REFLEX
(doll’s eyephenomenon)
• Brisk turning of the head from middle position to 90° on both
sides.
• In BD- no eye movements are observed.
• The neural pathways are mediated through arcs involving the
vestibular mechanisms, medial longitudinal fasciculus (brain
stem), and ocular nerves.
• Must not be performed in patients with an unstable cervical
spine.
34.
OCULOVESTIBULAR REFLEX
• Confirmthat in both ears, the tympanic membranes are intact and
that the external auditory canal is not obstructed.
• Obstructed EAC →impair the response
• Perforated eardrum→ augments the response
• In perforated eardrum, the test can be performed using cold air as
the stimulus.
• A fracture of the base of skull resulting in blood, cerebrospinal fluid
or brain tissue in the external auditory canal is a contraindication
35.
• Patient’s head: centre and lifted 30 degree from the supine
position.
• A soft catheter introduced into the EAC and slow irrigation with
10- 50 ml of ice cold water is performed while the eyes are held
‑
open by an assistant.
• The eyes are observed for one minute after the irrigation is
completed before repeating the test on the other side
• INTACT -tonic deviation of the eyes opposite to that of the
irrigated ear
• BRAIN DEAD -eyes remain fixed
37.
• Severe facialand ocular trauma, eyelid oedema, and chemosis
of the conjunctiva → limit movement of the globes → very
difficult to elicit and observe eye movements.
• Drugs that can lessen this reflex, such as tricyclic
antidepressants, aminoglycosides, antiepileptic drugs,
anticholinergics, and chemotherapeutic agents
• A combined ice cold water caloric stimulation and head
‑
rotation testing has been suggested as the most profound
stimulation for deeply unconscious patients
38.
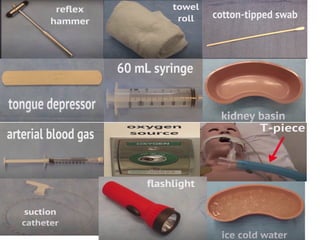
GAG REFLEX
• Atongue depressor is used to stimulate each side of the oropharynx
and the patient observed for any pharyngeal or palatal movement.
• Evaluation may be difficult in an intubated patient and should not
be performed if extubation is required to conduct the test.
COUGH REFLEX
• A suction catheter is introduced into the endotracheal or
tracheostomy tube to deliberately stimulate the carina.
• The patient is closely observed for any cough response or
movements of the chest or diaphragm.
40.
APNOEA TEST
• Doneafter documentation of coma, documentation of absent brain
stem reflexes, prerequisites have been met with.
Contraindication
• Associated high cervical cord injury, that abolished phrenic nerve
function
• Hemodynamic instability (arterial hypotension)
• Hypoxemia (pO2 <90 mmHg)
• Inability to achieve target PaCO2 levels
• Extensive thoracic trauma
• Significant pulmonary disorders interfering with ventilation
42.
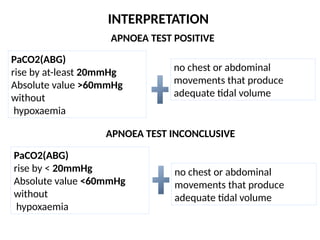
INTERPRETATION
no chest orabdominal
movements that produce
adequate tidal volume
PaCO2(ABG)
rise by at-least 20mmHg
Absolute value >60mmHg
without
hypoxaemia
APNOEA TEST POSITIVE
APNOEA TEST INCONCLUSIVE
no chest or abdominal
movements that produce
adequate tidal volume
PaCO2(ABG)
rise by < 20mmHg
Absolute value <60mmHg
without
hypoxaemia
43.
4
3
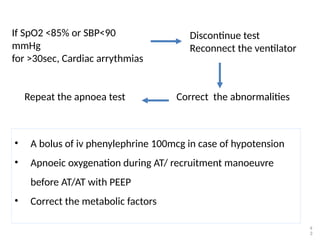
Discontinue test
Reconnect theventilator
If SpO2 <85% or SBP<90
mmHg
for >30sec, Cardiac arrythmias
Correct the abnormalities
Repeat the apnoea test
• A bolus of iv phenylephrine 100mcg in case of hypotension
• Apnoeic oxygenation during AT/ recruitment manoeuvre
before AT/AT with PEEP
• Correct the metabolic factors
44.
• The exactlevel of Paco2 to be achieved is still unknown, but the
American Academy of Neurology criteria adopt the level of
Paco2 60 mm Hg or greater
• The U.K. criteria requires a Paco2 target of 6.65 kPa (50 mm Hg)
• Assessment of neurologic function may be unreliable
immediately after cardiopulmonary resuscitation or other
severe acute brain injuries, and evaluation for brain death
should be deferred for 24 to 48 hours or longer if concerns exist
or inconsistencies are found in the examination
46.
Observations which arecompatible and
incompatible with brain stem death
Compatible:
• Spinal reflexes
• Sweating, blushing, tachycardia
• Normotension without pharmacologic support
• Absence of diabetes insipidus (DI).
Incompatible:
• Decerebrate or decorticate posturing
• Extensor or flexor motor responses to painful stimuli
• Seizures
47.
CONFIRMATORY / ANCILLARYTESTS
• THESE TESTS ARE CONDUCTED WHEN THE CLINICAL
EXAMINATION CANNOT BE PERFORMED FULLY AS IN SEVERE
CASES OF FACIAL TRAUMA OR SWELLING OR IF APNOEA TEST
CANNOT BE COMPLETED DUE TO HYPOXIA OR HEMODYNAMIC
INSTABILITY DURING THE TEST OR INCONCLUSIVE.
• Testing of cerebral perfusion is the preferred method of ancillary
testing.
• Recommended in children <1 year
4
7
48.
These tests areas follows:
– CEREBRAL ANGIOGRAM
– TRANSCRANIAL DOPPLER
– ELECTROENCEPHALOGRAM
– RADIONUCLIDE SCANS
– ATROPINE TEST
49.
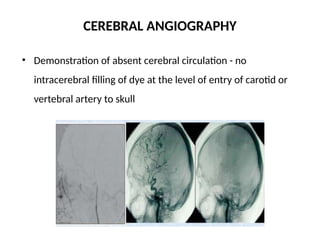
CEREBRAL ANGIOGRAPHY
• Demonstrationof absent cerebral circulation - no
intracerebral filling of dye at the level of entry of carotid or
vertebral artery to skull
50.
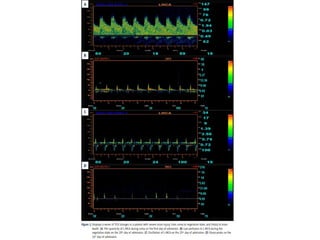
TRANSCRANIAL DOPPLER
• Highlysensitive to determine absent cerebral perfusion
• TCD examination has advantage over EEG for patients treated
with sedative drugs because TCD is not affected by them.
• The occurrence of RDF, early sharp systolic peaks of forward
flow (sharp peaks), and disappearance of blood flow may
suggest an onset of brain death
52.
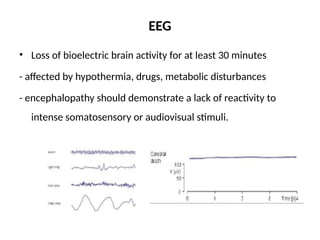
EEG
• Loss ofbioelectric brain activity for at least 30 minutes
- affected by hypothermia, drugs, metabolic disturbances
- encephalopathy should demonstrate a lack of reactivity to
intense somatosensory or audiovisual stimuli.
53.
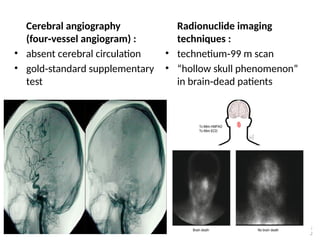
Cerebral angiography
(four vesselangiogram) :
‑
• absent cerebral circulation
• gold standard supplementary
‑
test
Radionuclide imaging
techniques :
• technetium 99 m scan
‑
• “hollow skull phenomenon”
in brain dead patients
‑
5
3
54.
5
4
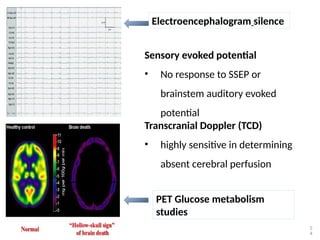
Electroencephalogram silence
Sensory evokedpotential
• No response to SSEP or
brainstem auditory evoked
potential
Transcranial Doppler (TCD)
• highly sensitive in determining
absent cerebral perfusion
PET Glucose metabolism
studies
55.
NEGATIVE ATROPINE TEST
•Assesses bulbar parasympathetic activity on heart activity in
brain-dead patients
• Inject 2 mg atropine under continuous monitoring of the ECG
during 10 minutes.
• Test is negative if heart rate is not augmented by more than 3%
compared with basal ECG record.
5
5
56.
• If theancillary study supports the diagnosis, the second
examination and apnoea testing can then be performed.
• When an ancillary study is used to reduce the observation
period, all aspects of the examination and apnoea testing should
be completed and documented.
5
6
57.
Criteria for DiagnosingBrain Death in Infants and
Children
• As children are more resilient than adults, a longer time
between assessments, of greater than 6 hours, has been
advocated.
• Term to 2 months old: 48 hours,
• >2 months to 1 year:24 hours,
• >1 year to <18 years: 12 hours,
• >18 year: As in adults.
58.
• The diagnosisof brain death cannot be made in preterm
infants of gestational age of less than 37 weeks.
• Assessments in neonates and infants should be performed by
pediatric specialists with critical care training
59.
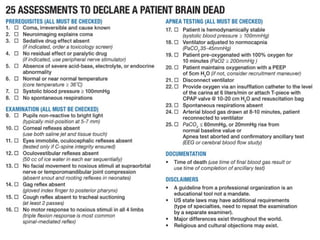
What needs tobe included in medical record
documentation?
All phases of the determination of brain death should be clearly
documented in the medical record:
• Etiology and irreversibility of coma/unresponsiveness
• Absence of motor response to pain
• Absence of brain stem reflexes during two separate
examinations separated by at least 6 h
• Absence of respiration with pCO2 ≥60 mmHg
• Justification for, and result of, confirmatory tests if used
5
9
61.
CERTIFICATION OF BRAINDEATH
• THOA Act, 1994 (sub sec 6 of sec 3), Brainstem death refers to
“stage at which all functions of the brain stem have
permanently and irreversibly ceased”
• RMP – do apnea test and certify
• Diagnosis is established and recorded by 2 doctors not
belonging to retrieval and transplantation team.
• Out of the 2 doctors, one must be a neurologist
• The order of examination is irrelevant
62.
EVALUATION TEAM
• Certificationrequired board of medical experts consisting of:
1. Doctor in charge of the patient
2. Doctor in charge of the hospital/MS
3. An independent medical practitioner nominated by MS of
the hospital
4. Neurologist/neurosurgeon nominated by the MS
• Form 10 should be filled & signed
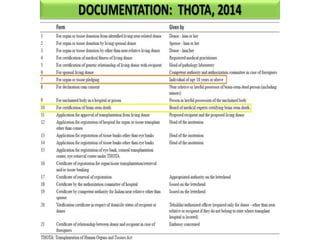
64.
• THOA 2011& 2014 – allowed surgeon/physician and
anaesthetist /intensivist if non availability of
neurosurgeon/neurologist
• Clinical examination and apnoea test to be done 2 times after
an interval of 6 hours
• After the second test, counsel the family regarding organ
donation
• The time of death is the end of the second apnea test.
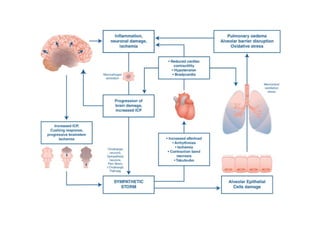
MECHANISM
• Brain injury– trauma, vascular injury, generalized hypoxia
• Brain edema – vasogenic/cytotoxic
– Vasogenic – destroyed BBB increases permeability
– Cytotoxic – disturbance of cellular osmoregulation (aquaporins)
• Initially focal brain edema later spreads throughout the whole
brain
• After 3- 6 days – aseptic necrosis of brain
• 2 patterns regarding CBF – 1. CPP 0 due to raised ICP/CPP
maintained but primary metabolic failure of brain
67.
Neurophysiologic basis
• Irreversiblecessation of functioning of brain, but does not
require cessation of every neuron.
• Below C2 not included as they are spared from compression
during brain edema
68.
Respiratory centres
• Primarycentre – reticular core of medulla
• In brain death – no spontaneous respiration when PaCO2
reaches 55 – 60 mmHg
• Complete apnoea
• Mechanical stimulation of carina – cough reflex – detects
residual function of medullary neurons
Cardiovascular system
• Neuronsof circulatory system are diffusely located in pons
&medulla reticular core.
• Vasomotor & cardio accelerating neurons – negative
feedback control.
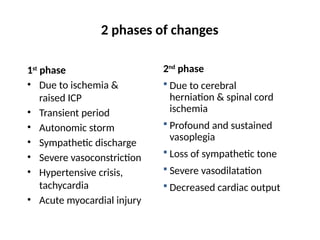
73.
1st
phase
• Due toischemia &
raised ICP
• Transient period
• Autonomic storm
• Sympathetic discharge
• Severe vasoconstriction
• Hypertensive crisis,
tachycardia
• Acute myocardial injury
2nd
phase
Due to cerebral
herniation & spinal cord
ischemia
Profound and sustained
vasoplegia
Loss of sympathetic tone
Severe vasodilatation
Decreased cardiac output
2 phases of changes
74.
• Vasomotor &cardioaccelerating neurons of spinal cord obtain
automaticity after several days – normal BP
• Autonomic spinal cord reflexes develop
• Lazarus sign – bizarre seemingly purposeful movements of the
upper extremities, in which the arms are flexed quickly to the
chest from the patient’s side, the shoulders adducted and in
some patients, the hands crossed or opposed below the chin.
75.
Regulation of bodytemperature
• Neuronal connection between hypothalamus &
peripheral body tissues are lost – poikilothermic.
• Temperature tends to be hypothermic even after
external heat application.
76.
Hypothalamo-pituitary endocrine system
•Hypothalamo-anterior pituitary function – preserved to a
certain degree for initial period
• Euthyroid sick syndrome (decreased T3 T4)
• Hyperglycemia – decreased insulin and increased insulin
resistance
• DIC – tissue thromboplastin release from brain
• Posterior pituitary function is not usually preserved
• Decreased ADH - DI
77.
Immune system
• Increasedcytokines – IL 1B, IL 6, TNF alpha, CAMs
• Acute phase reactants – low success rates after organ
transplantation
• SIRS
- inflammatory mediators from ischemic brain
- catecholamine induced anerobic metabolism
- Metabolic changes after brain death
- Neuropeptide release
78.
SUMMARY
• Patients withpoor GCS due to a known irreversible insult and in coma
can be considered for testing for brain death.
• Brain death is a clinical diagnosis made by demonstrating presence of
coma , absent brainstem reflexes and positive apnoea test (twice – 6
hours apart).
• If the apnoea test results are inconclusive ancillary testing can be done.
• Proper clinical testing and documentation should be done.
• Understanding the pathophysiological changes occuring following brain
death facilitates proper management of a donor.
• Caring of a potential donor is caring for multiple recepients!!