Downloaded 236 times



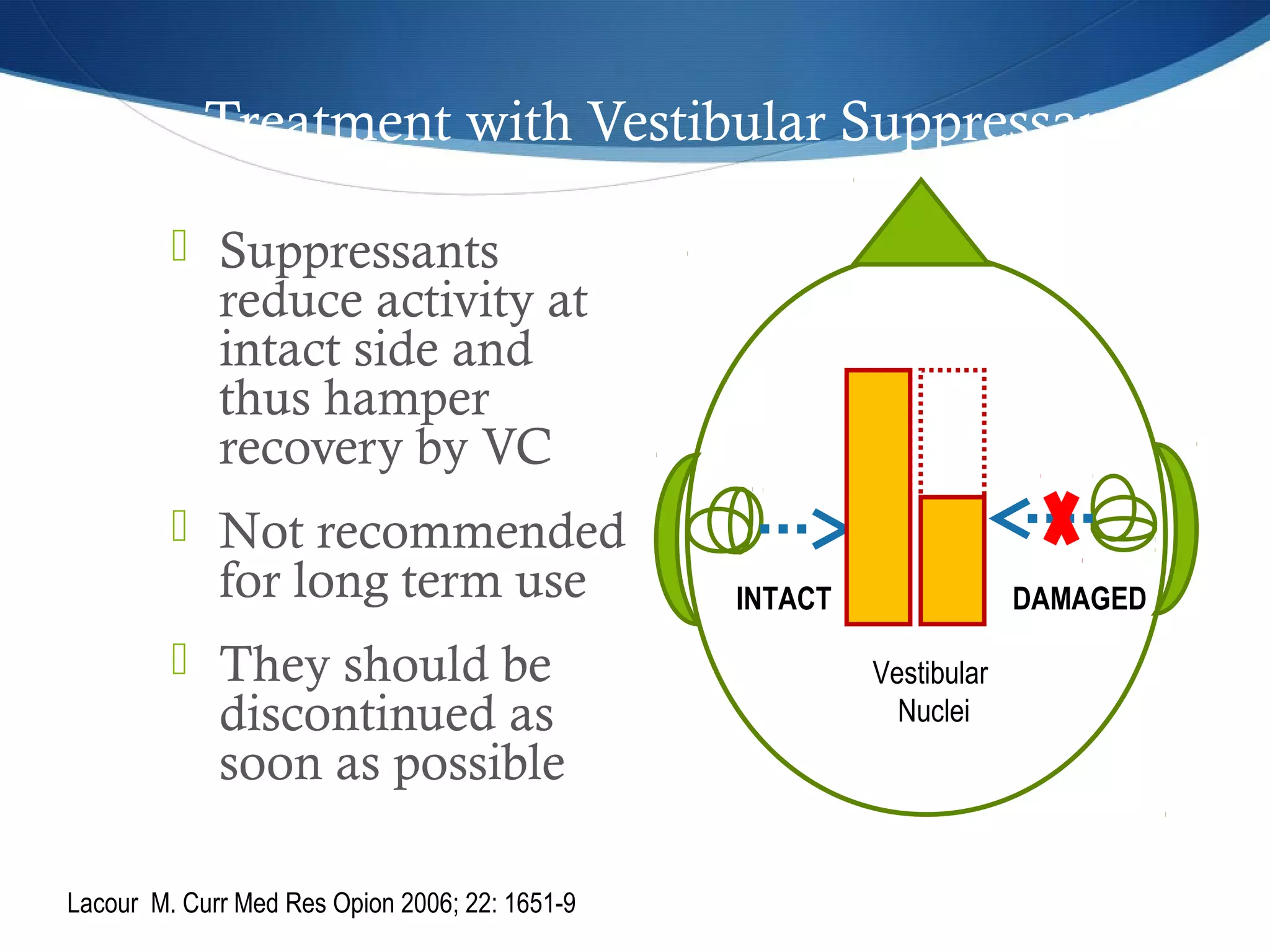
![CRANIOCORPOGRAPHY
Developed by Claussen [1968]
Assessment of vestibulospinal system
Photographic recording of head and body movement during
gait testing
Evaluation includes Romberg, Tandem walking and
Unterburger’s test](https://image.slidesharecdn.com/vertigo-makingitsimple-150212071851-conversion-gate02/75/Vertigo-making-it-simple-18-2048.jpg)
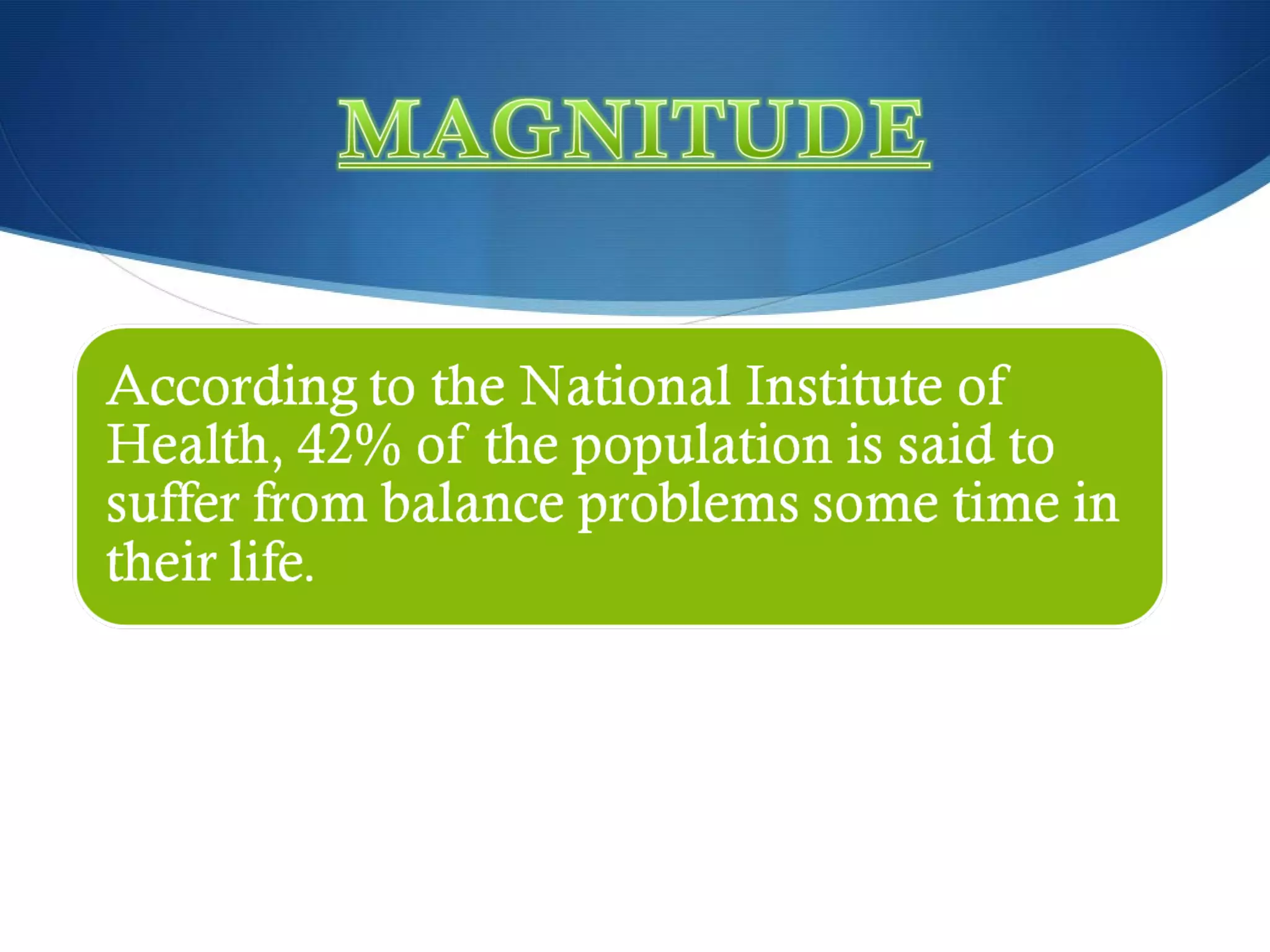
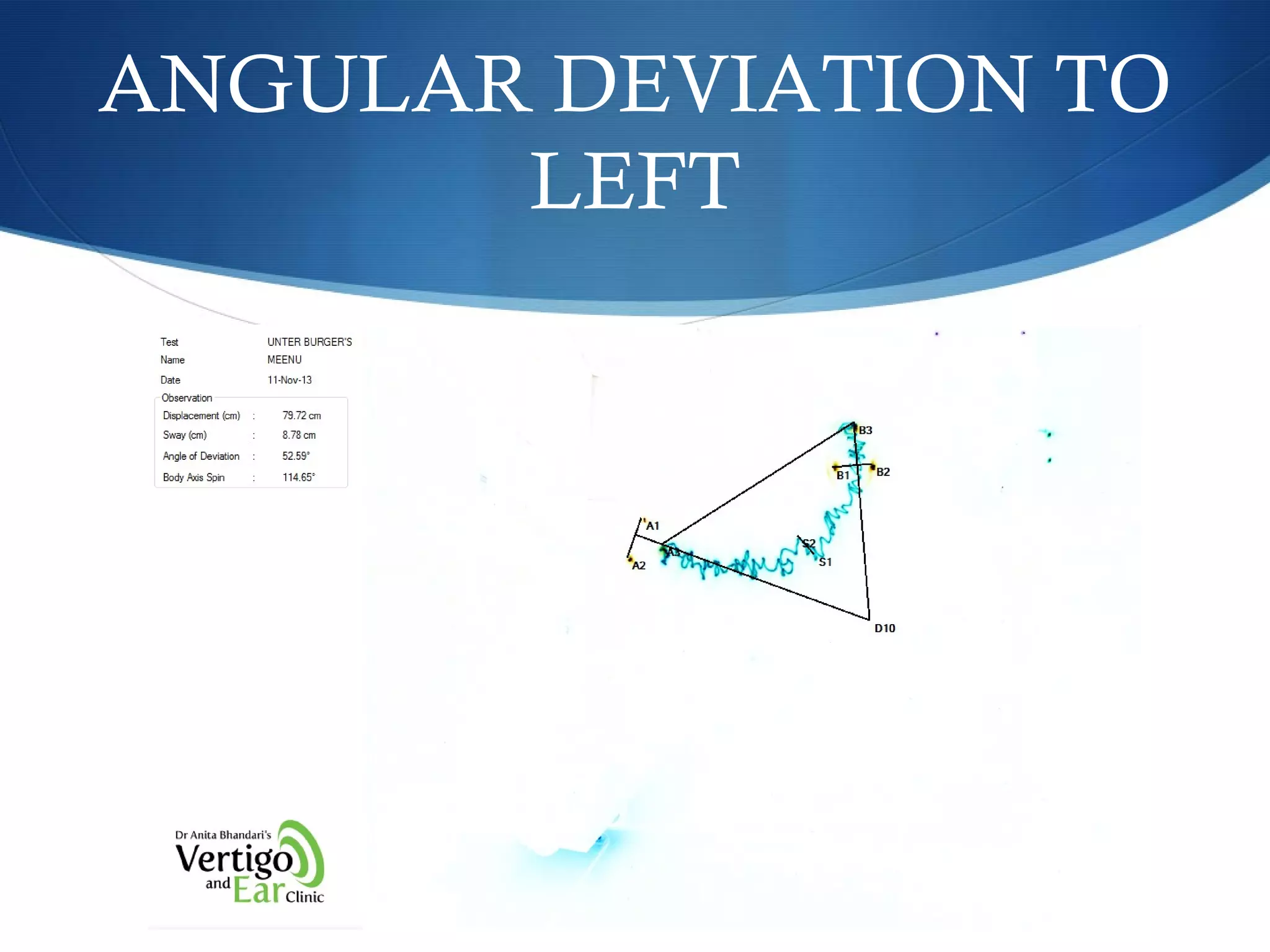
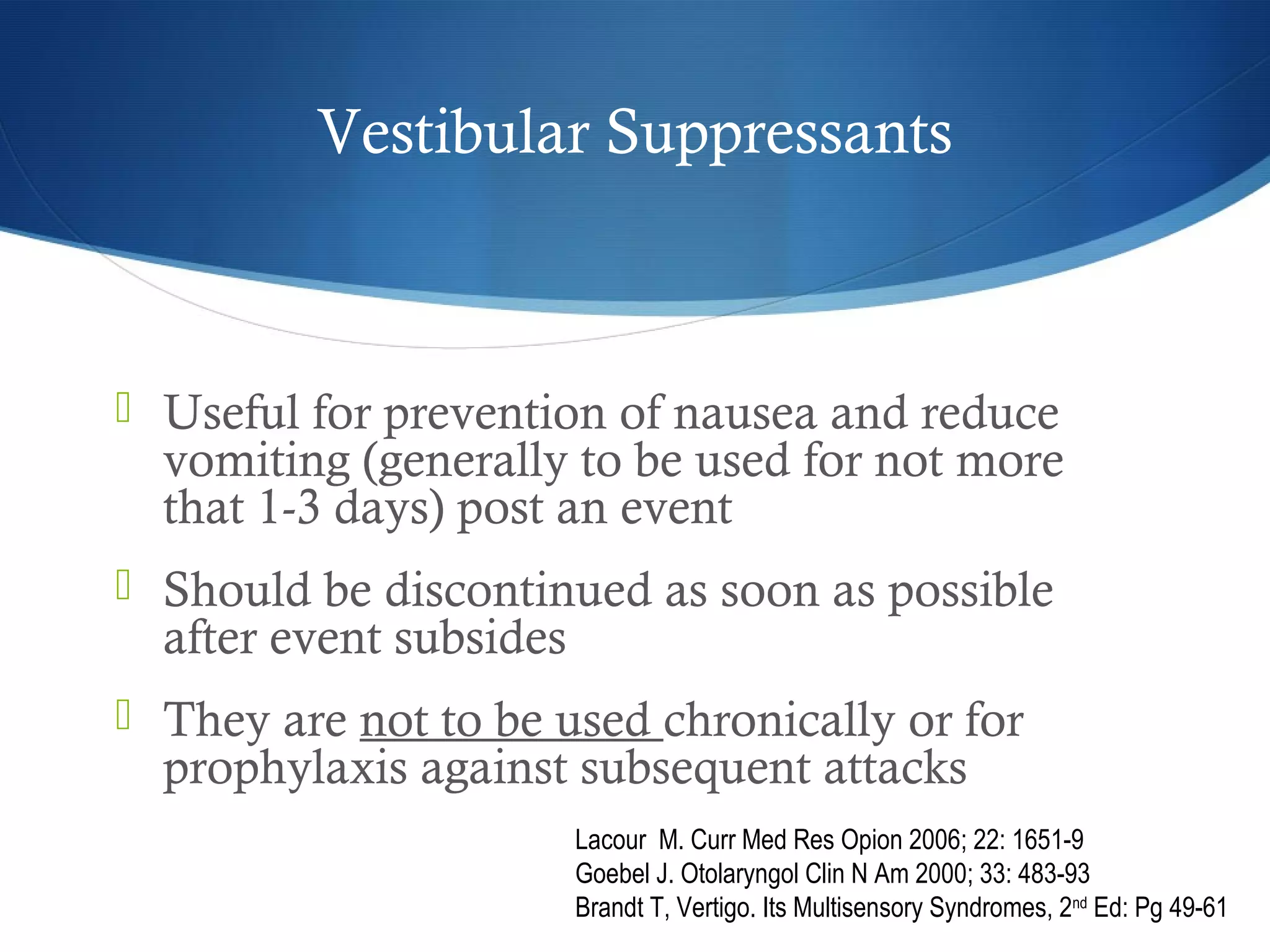
![PARAMETER NORMAL RANGE-
LOWER BORDER
NORMAL RANGE-
UPPER BORDER
Longitudinal
displacement
30.03 cm 113.35 cm
Lateral sway 5.17 cm 16.15 cm
Angular deviation 55.13° (right) 48.37° (left)
Body spin 82.21° (right) 82.89° (left)
NORMAL PARAMETER OF
CCG
[CLAUSSEN]](https://image.slidesharecdn.com/vertigo-makingitsimple-150212071851-conversion-gate02/75/Vertigo-making-it-simple-20-2048.jpg)
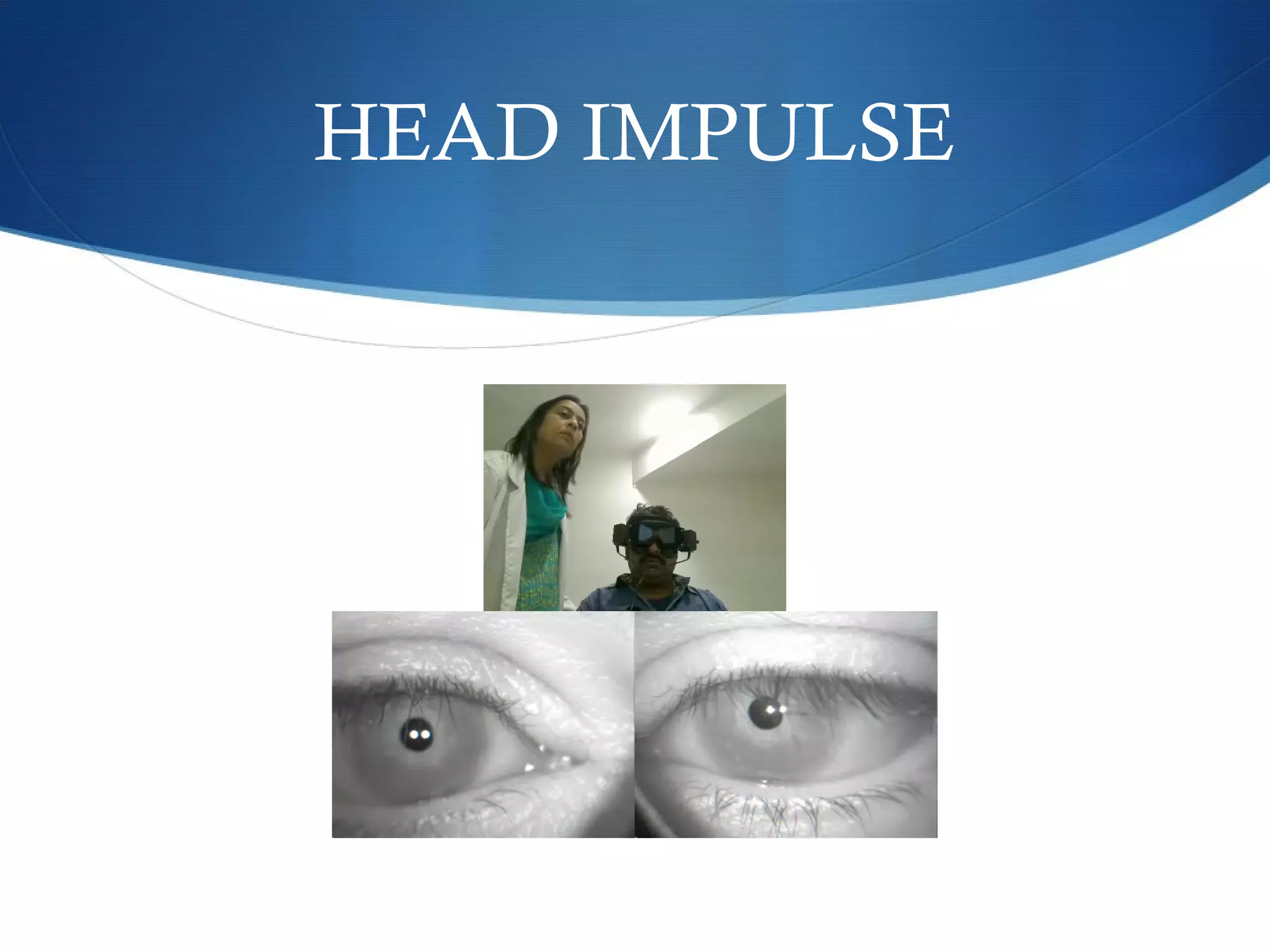
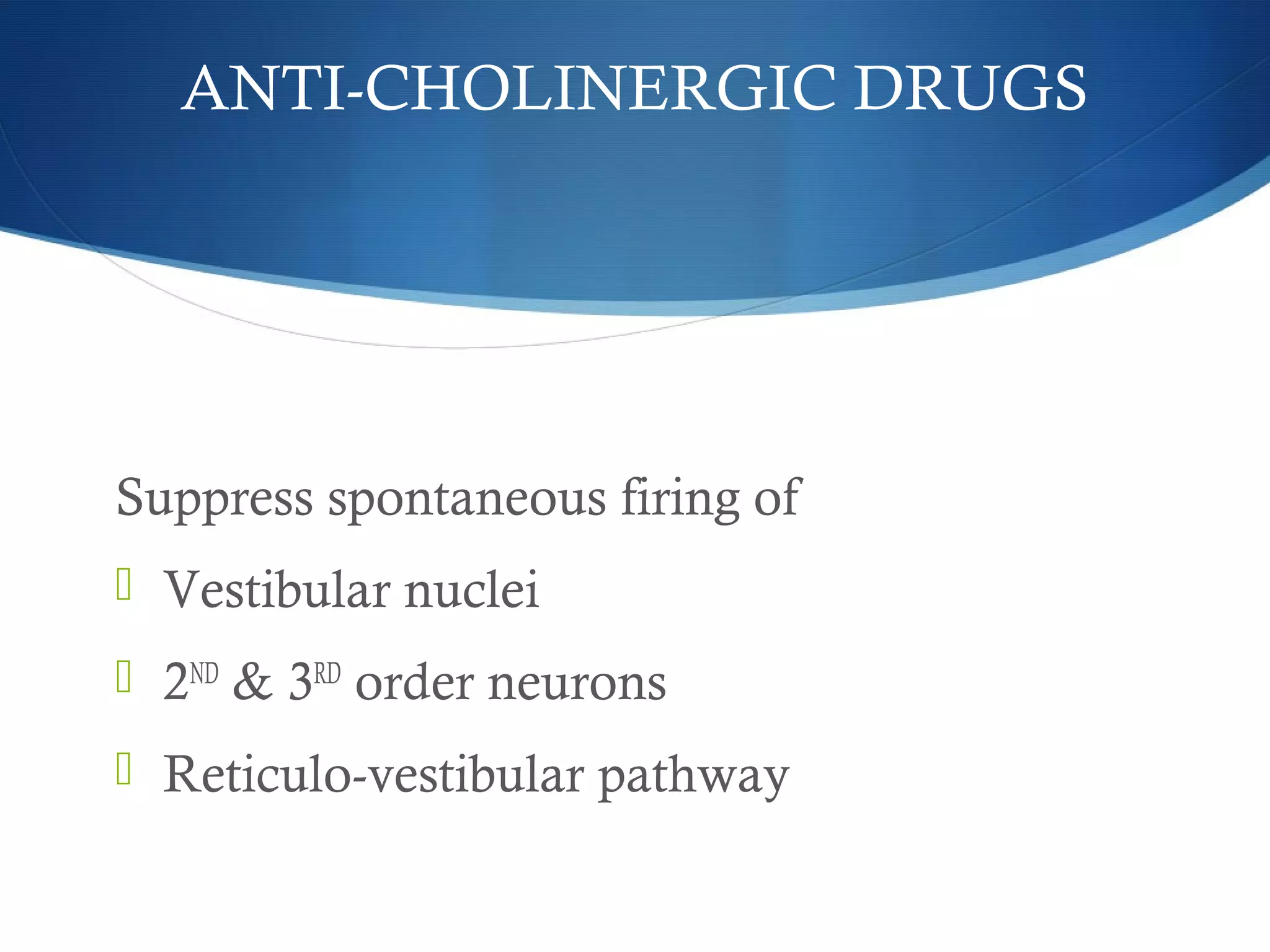
![ Subject seated upright with eyes focused on an fixed object
Unpredictable , low amplitude [10 – 20°] head rotation with
high acceleration
Angular VOR generates compensatory eye movements
equal in amplitude and opposite in direction to stabilize
gaze
HIT : PROCEDURE](https://image.slidesharecdn.com/vertigo-makingitsimple-150212071851-conversion-gate02/75/Vertigo-making-it-simple-27-2048.jpg)
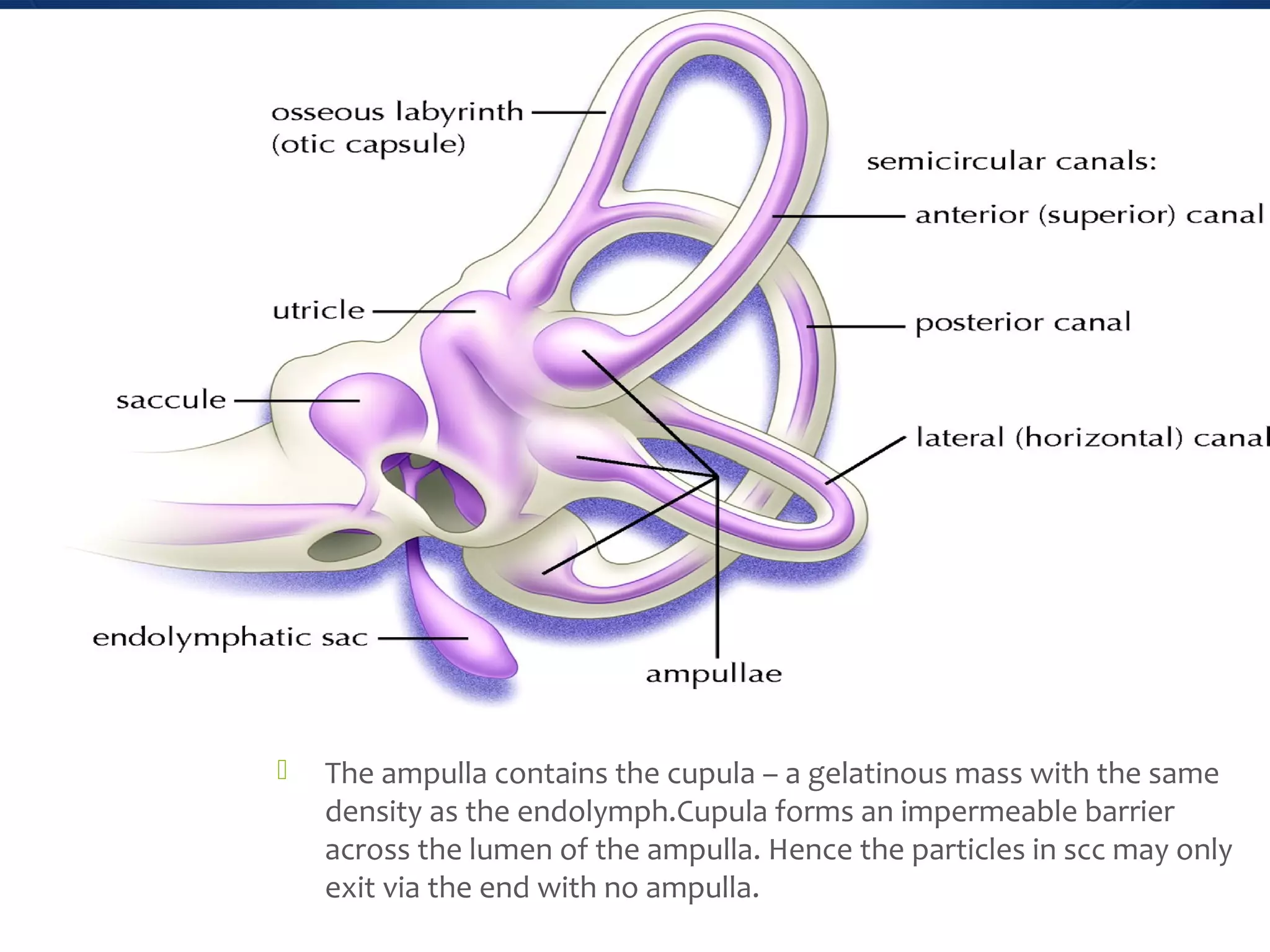
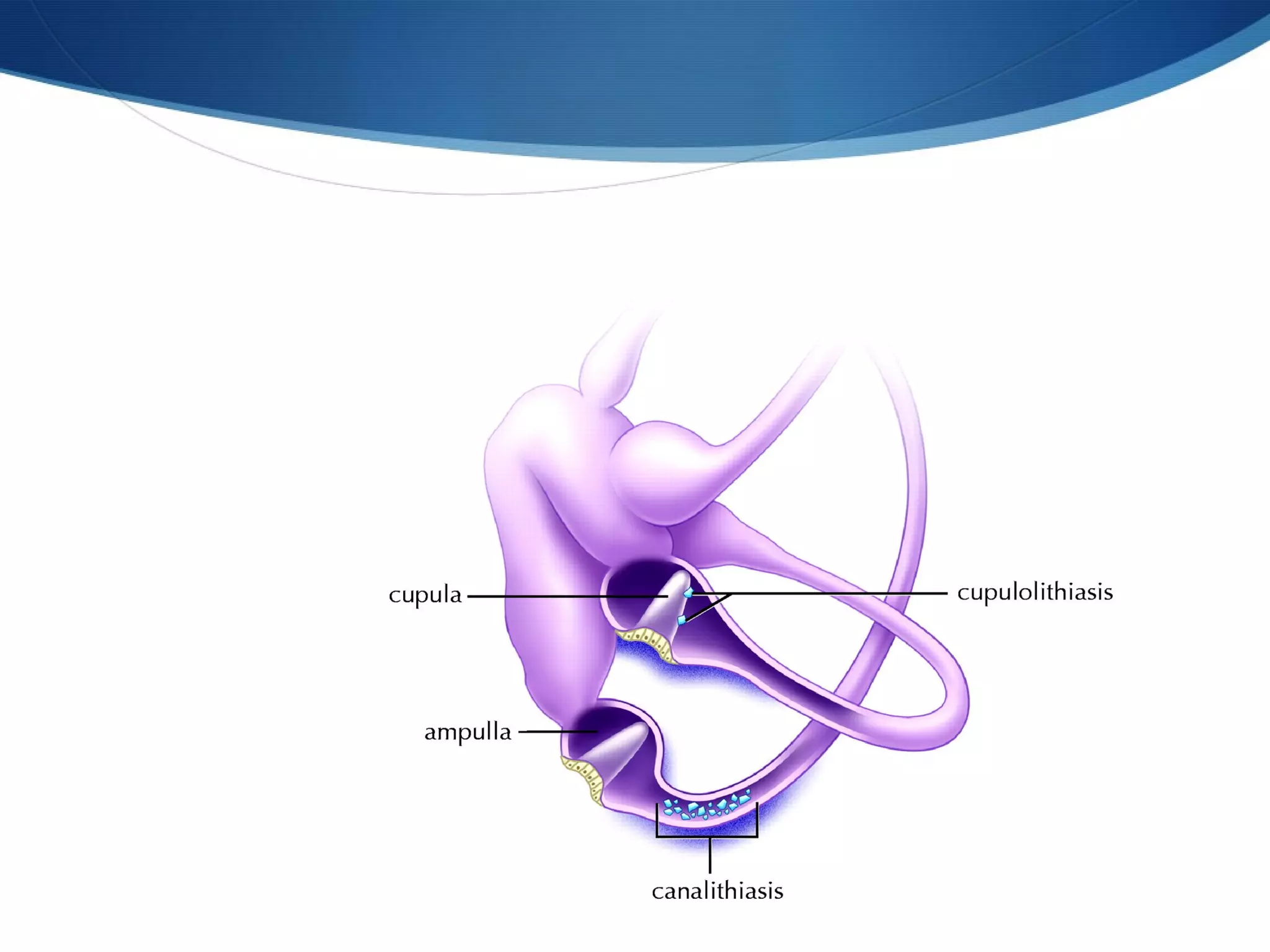
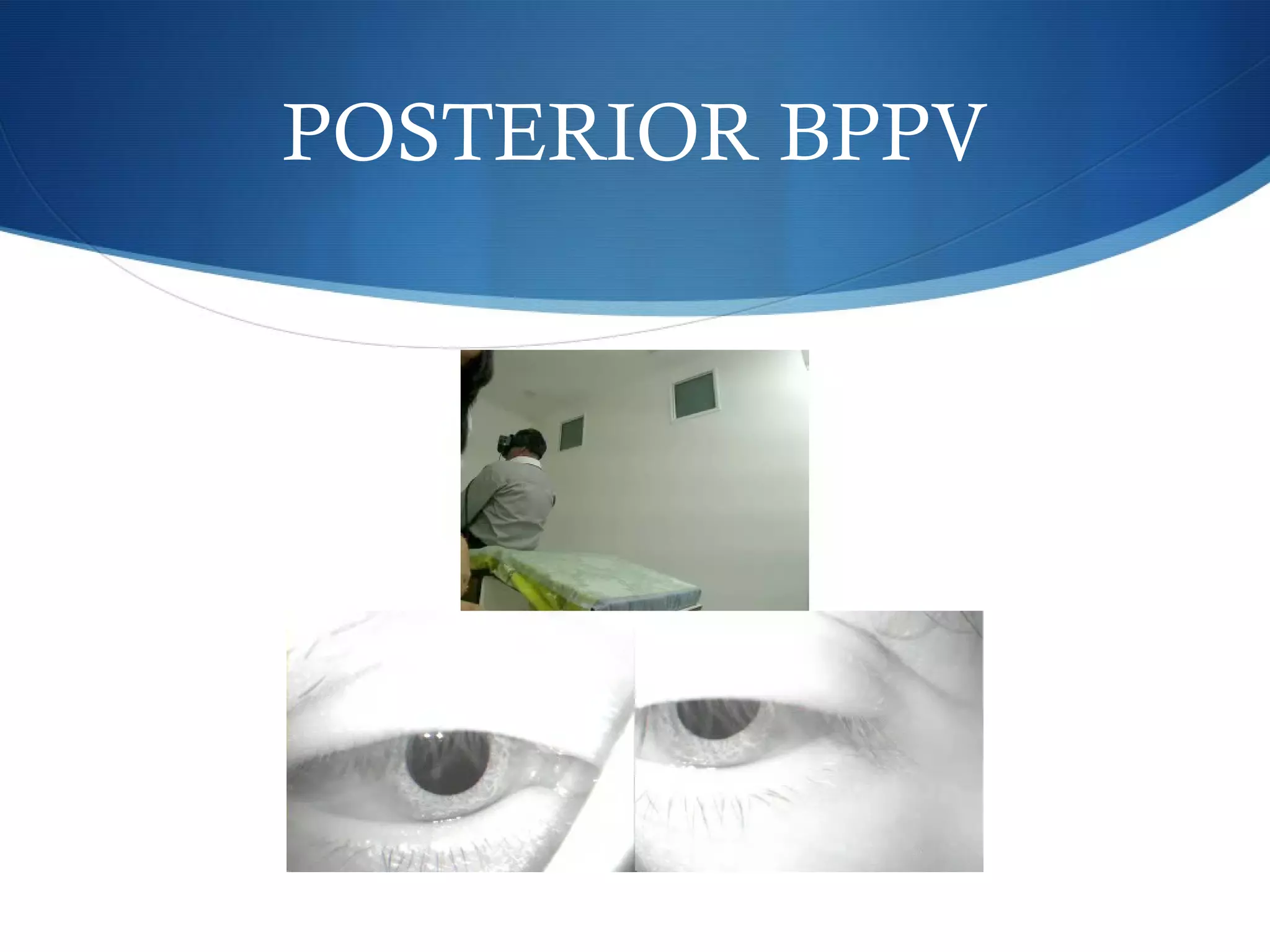
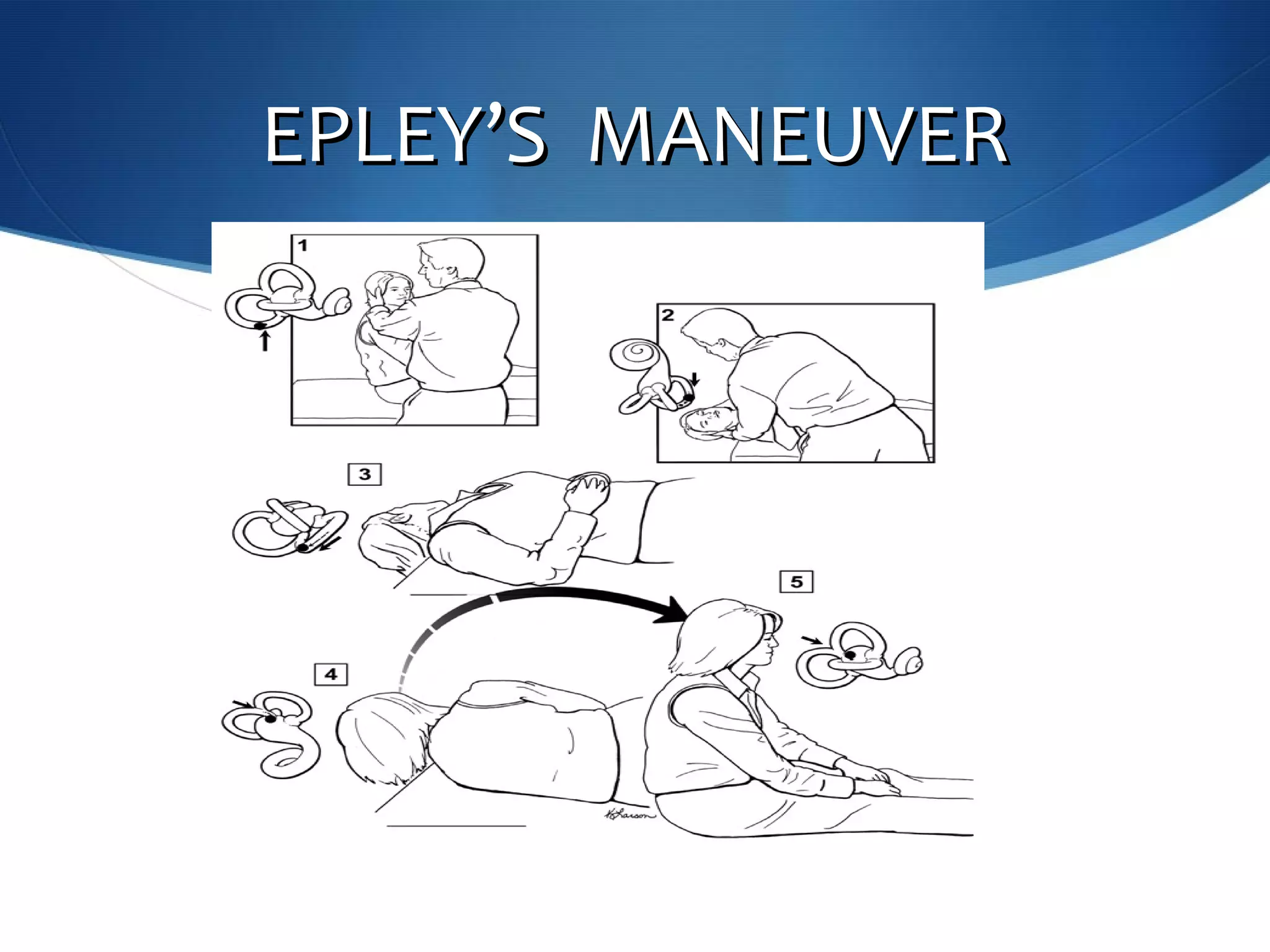
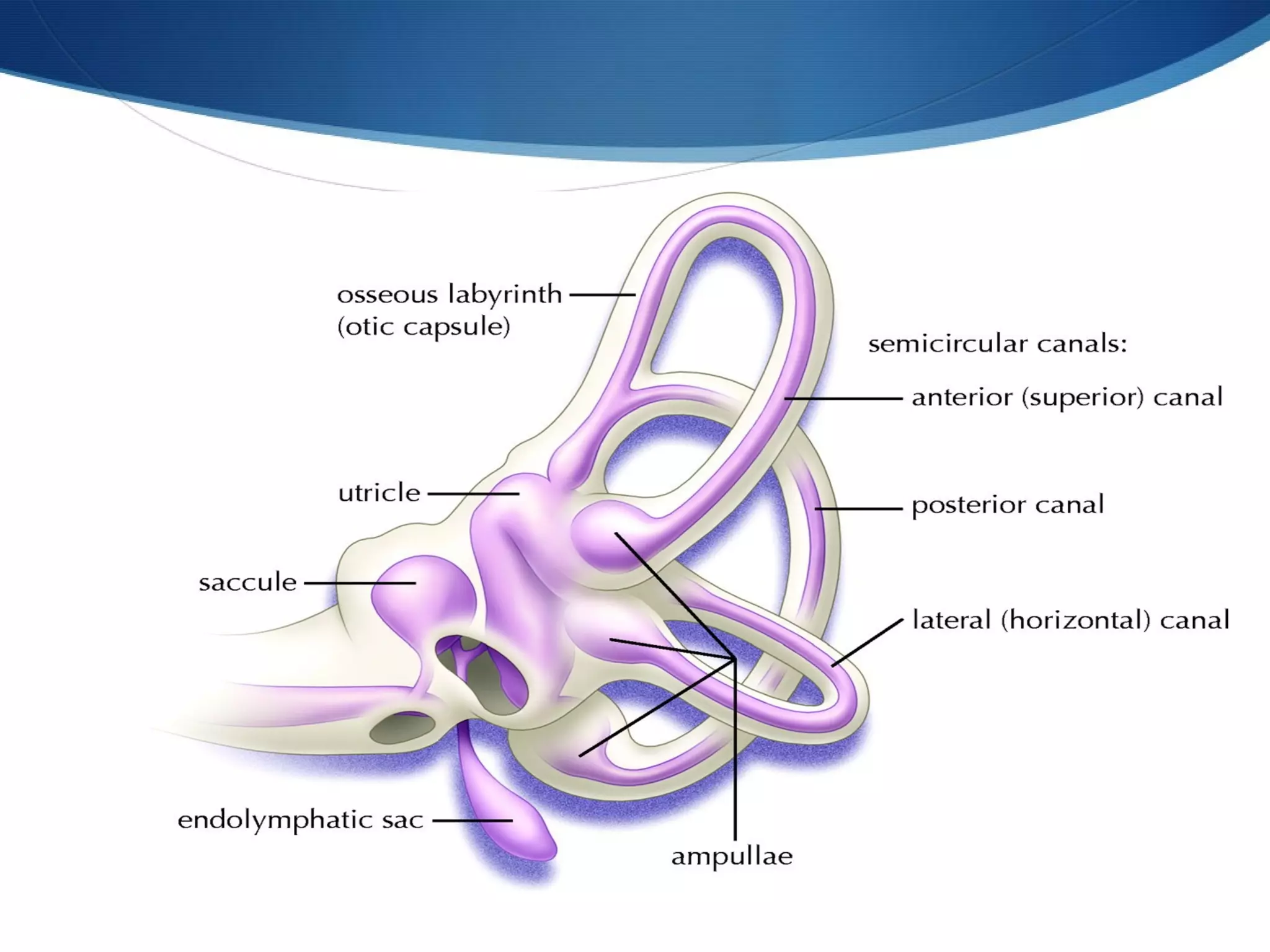
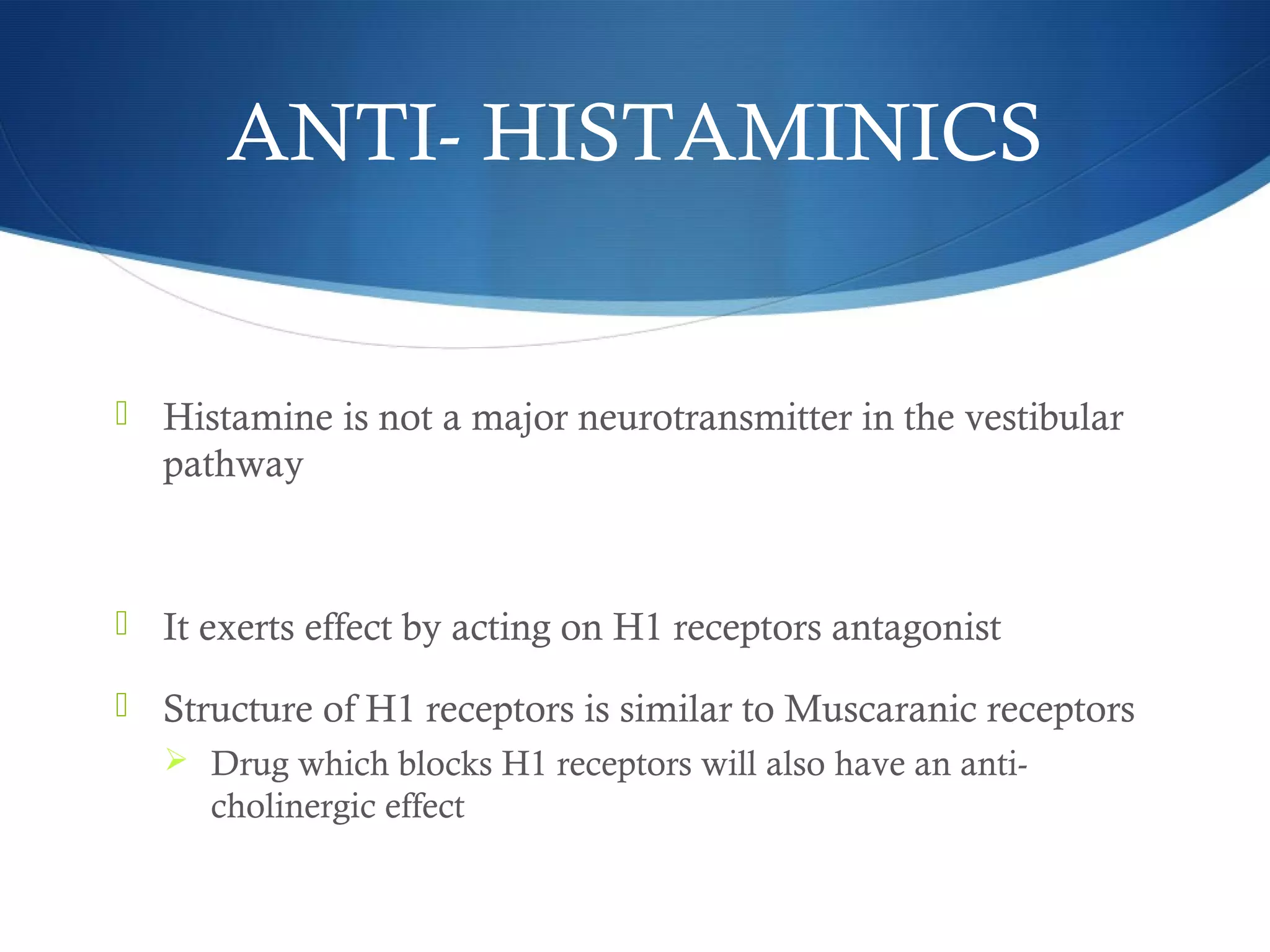
![POSTERIOR CANAL BPPVPOSTERIOR CANAL BPPV
Most common– posterior canal is most gravity dependent in
upright and supine position
Once debris enter the post. canal ,the cupula at the shorter
most dependent arm trap the debris.
Debris can exit only through the longer arm through the crus
commune [non-ampullary]](https://image.slidesharecdn.com/vertigo-makingitsimple-150212071851-conversion-gate02/75/Vertigo-making-it-simple-37-2048.jpg)
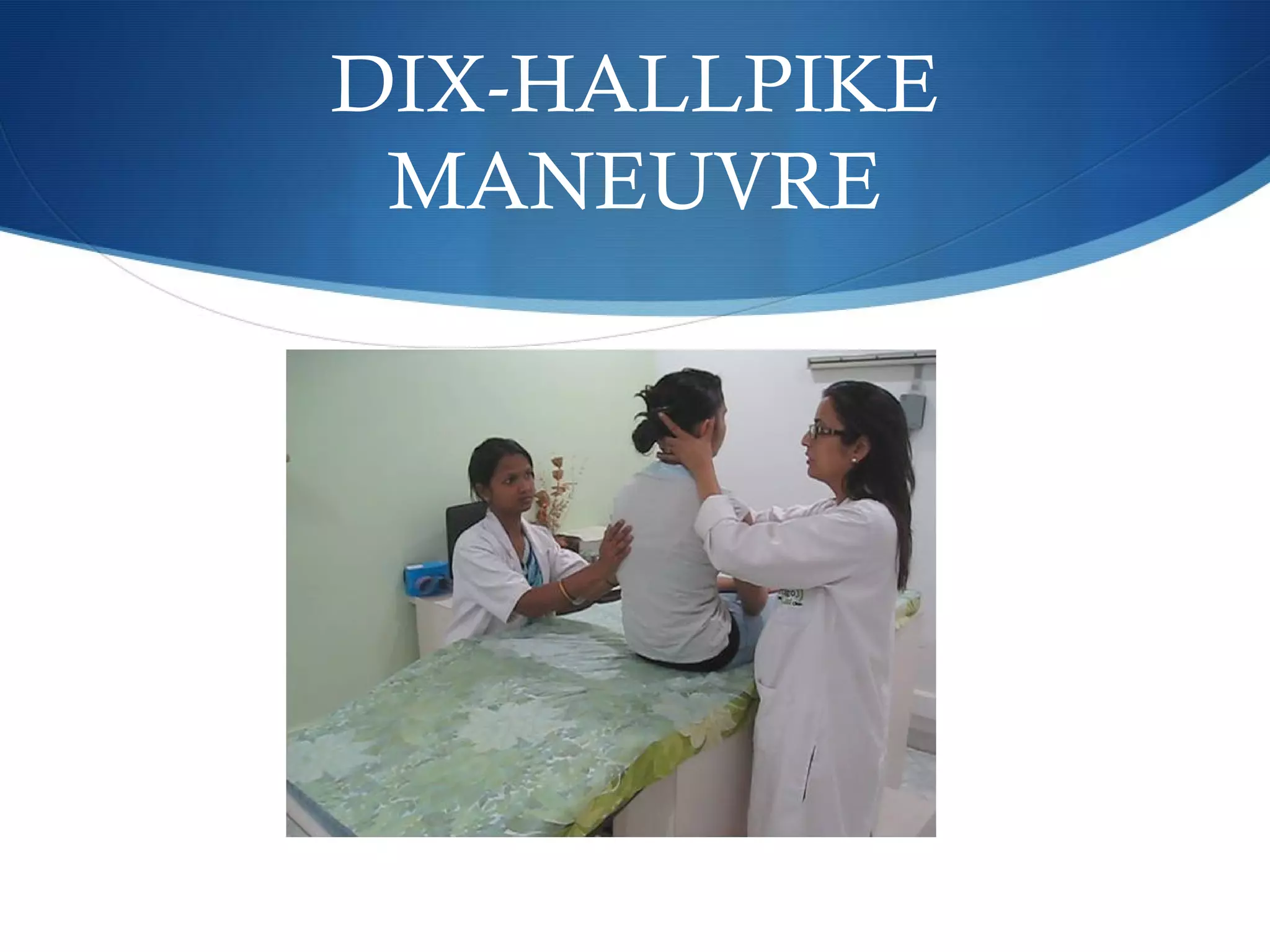





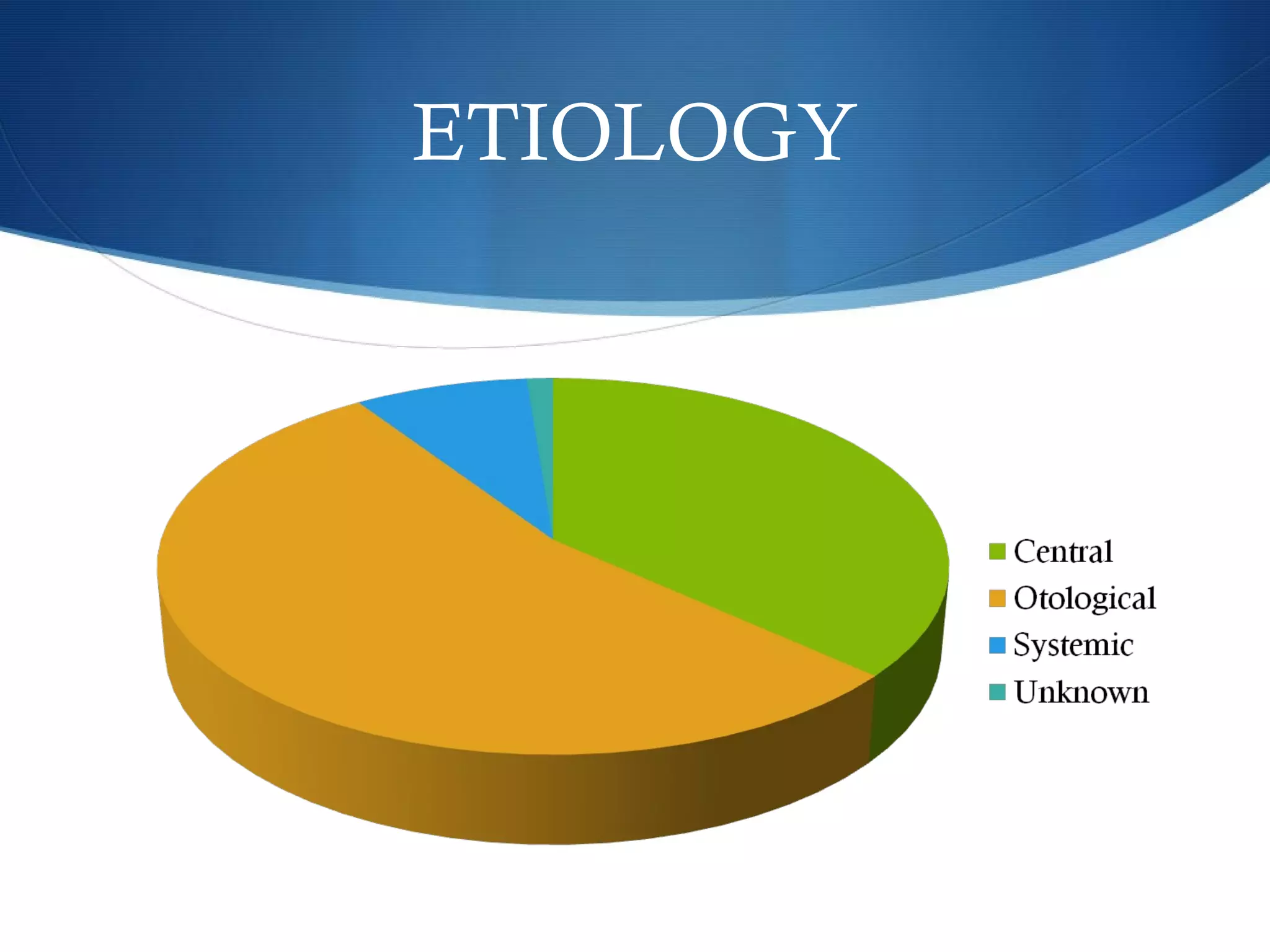
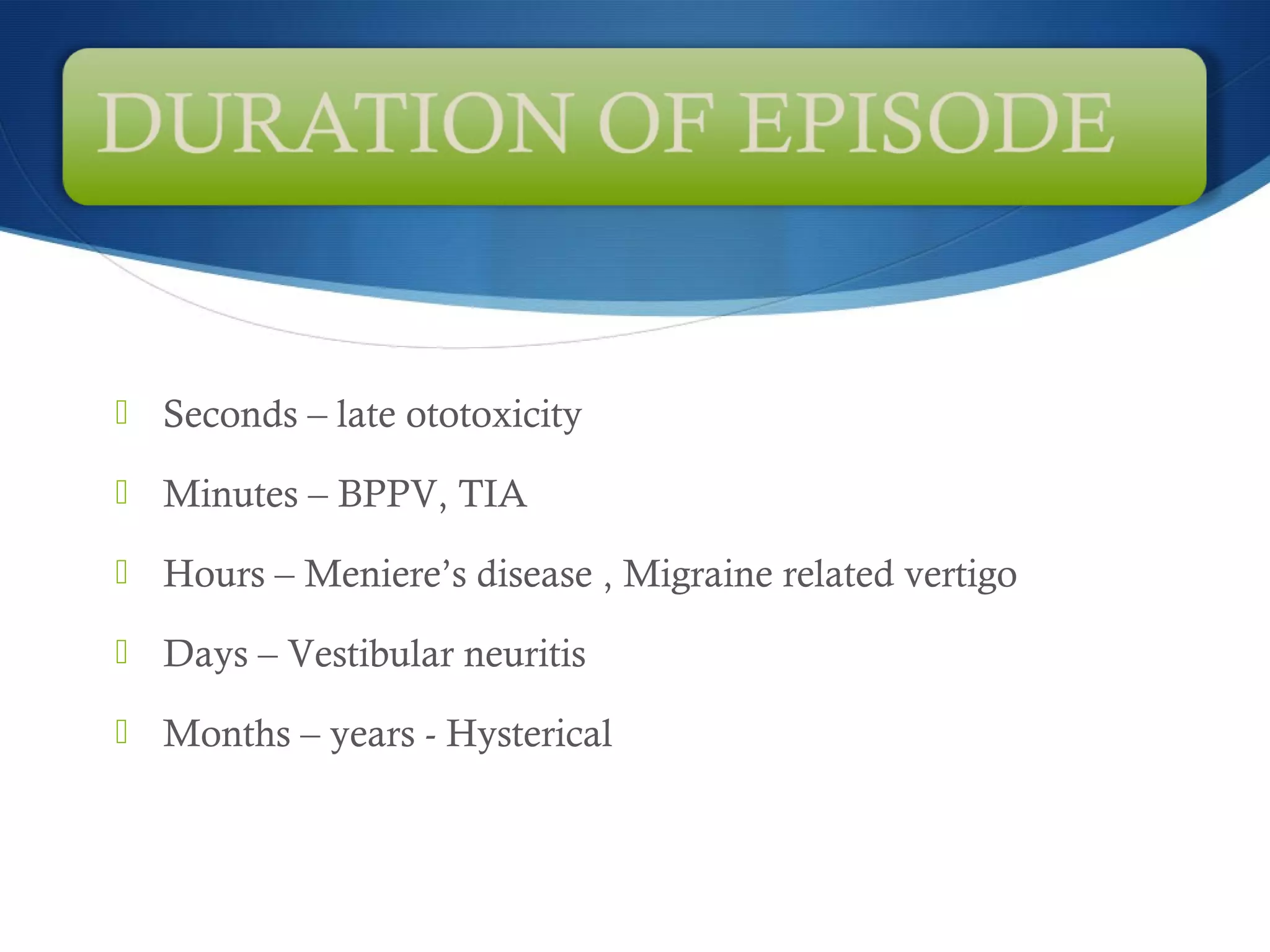
1) Vertigo can be caused by issues in the inner ear lasting seconds to years, with the most common causes being BPPV, vestibular neuritis, and Meniere's disease. 2) A neurotological evaluation includes tests of the vestibulo-ocular, vestibulospinal, and otolith systems like head impulse testing, caloric testing, and subjective visual vertical to locate the source of imbalance. 3) BPPV is diagnosed and treated with particle repositioning maneuvers like Epley and Semont maneuvers to move calcium carbonate debris out of the semicircular canals. Other causes like cupulolithiasis may require different treatments.









































































