
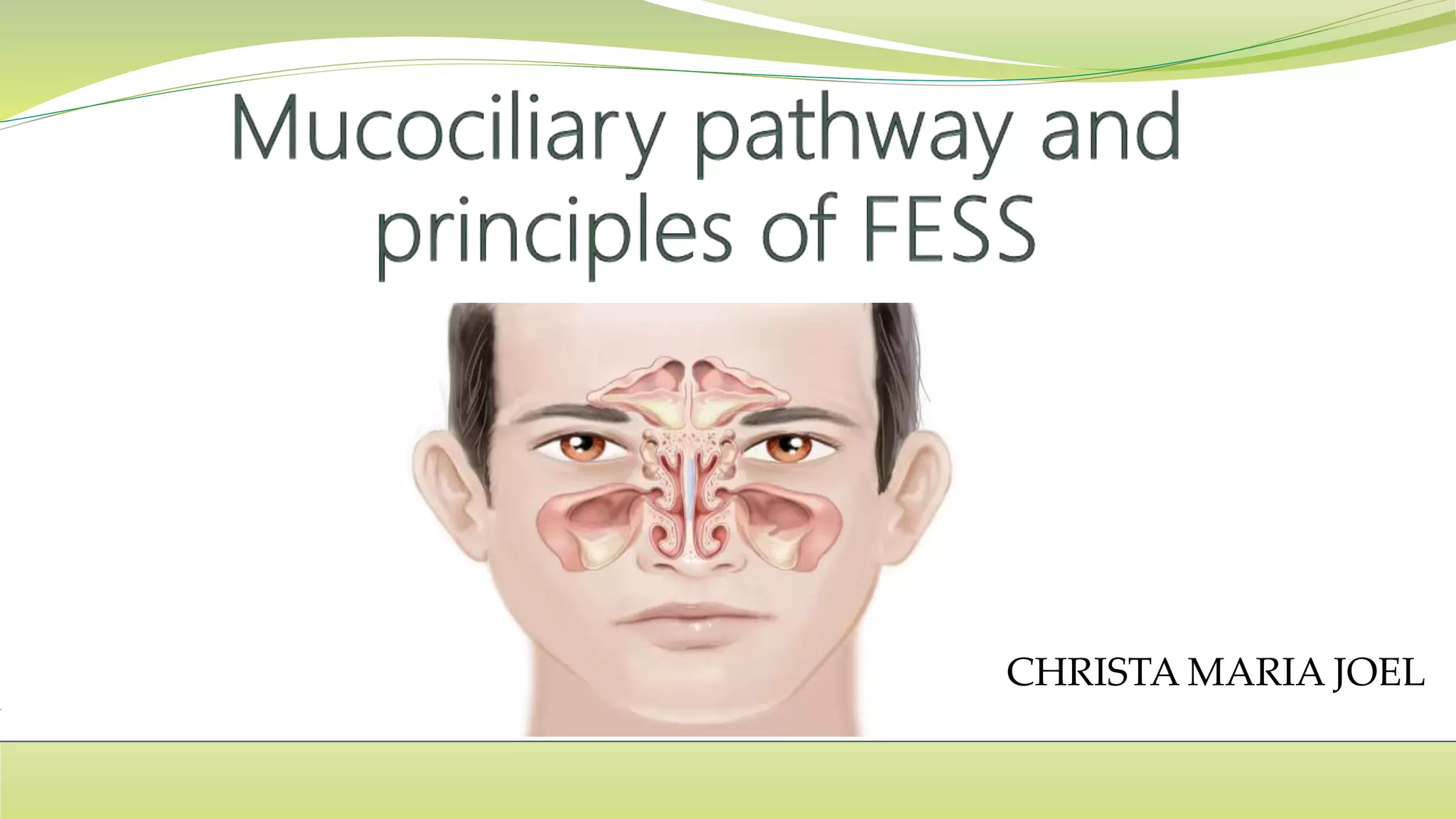
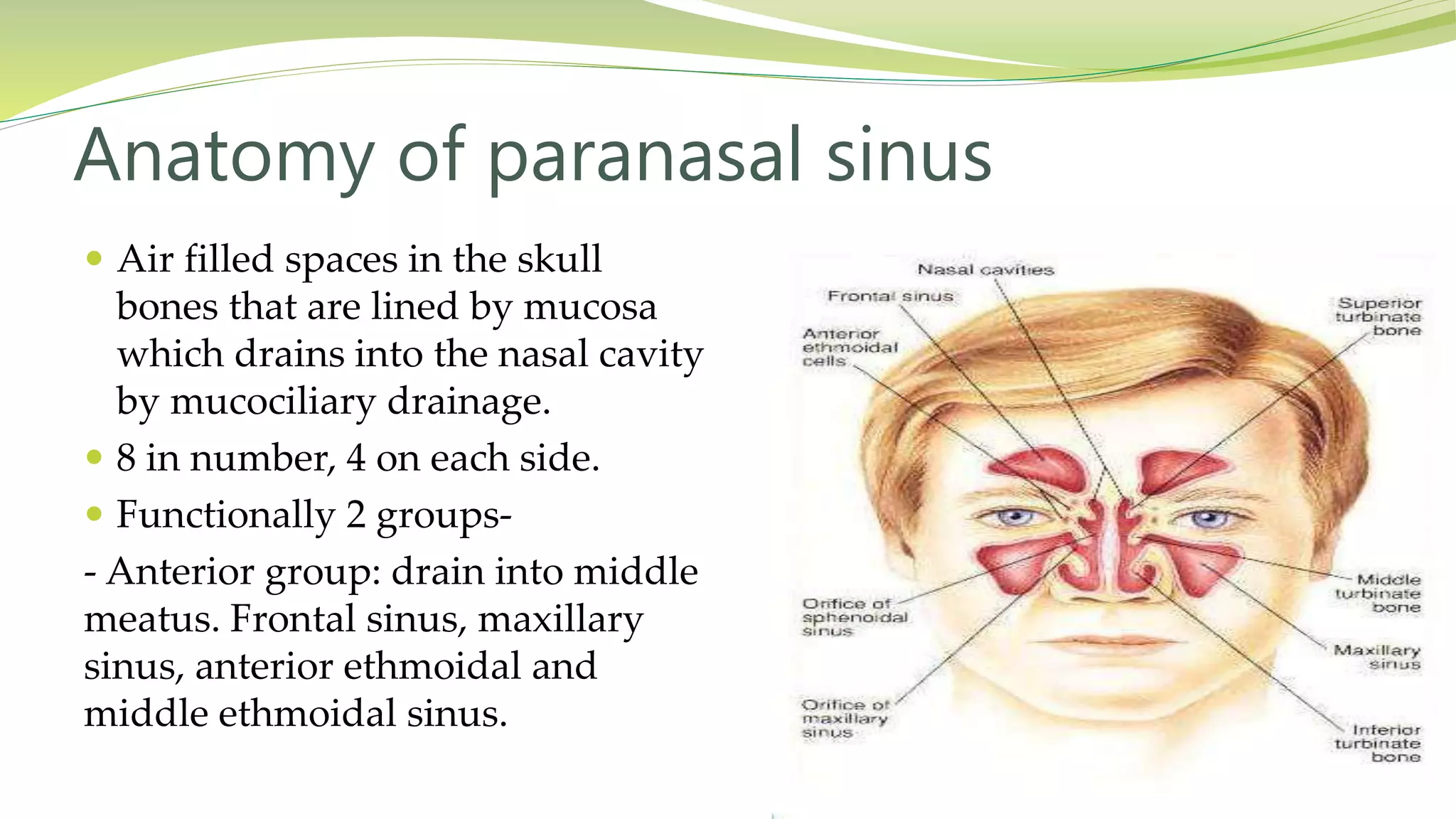
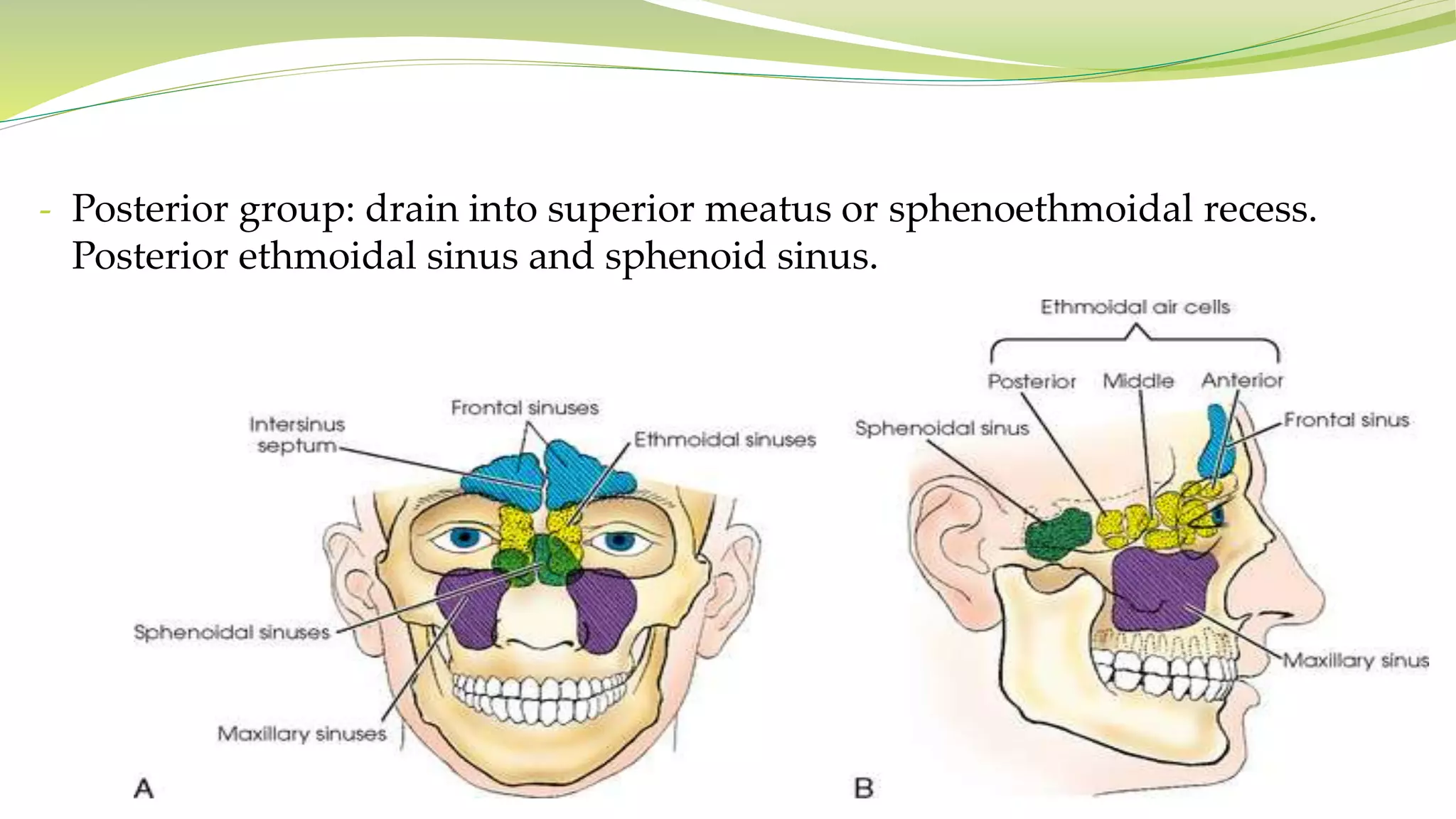
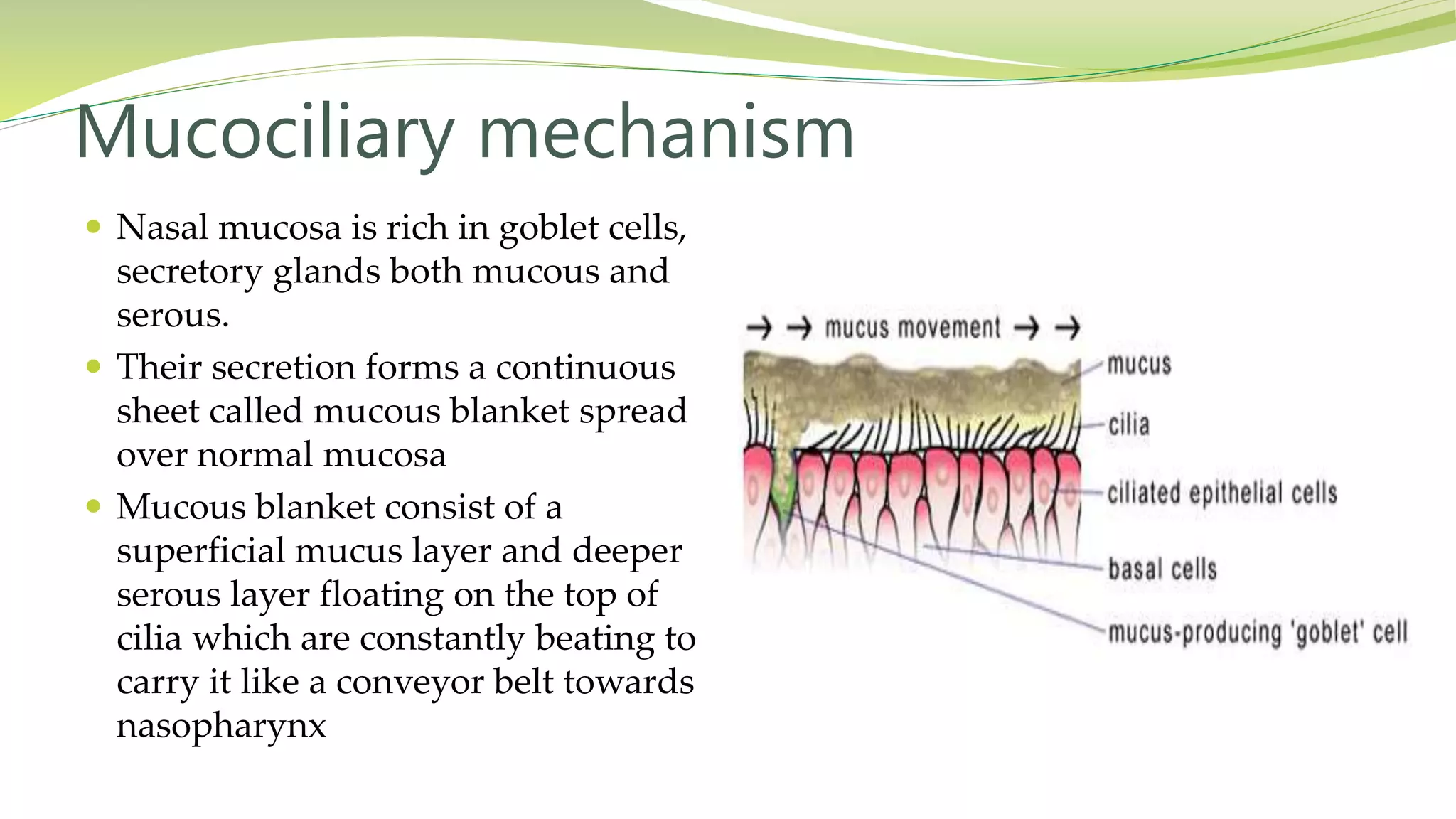
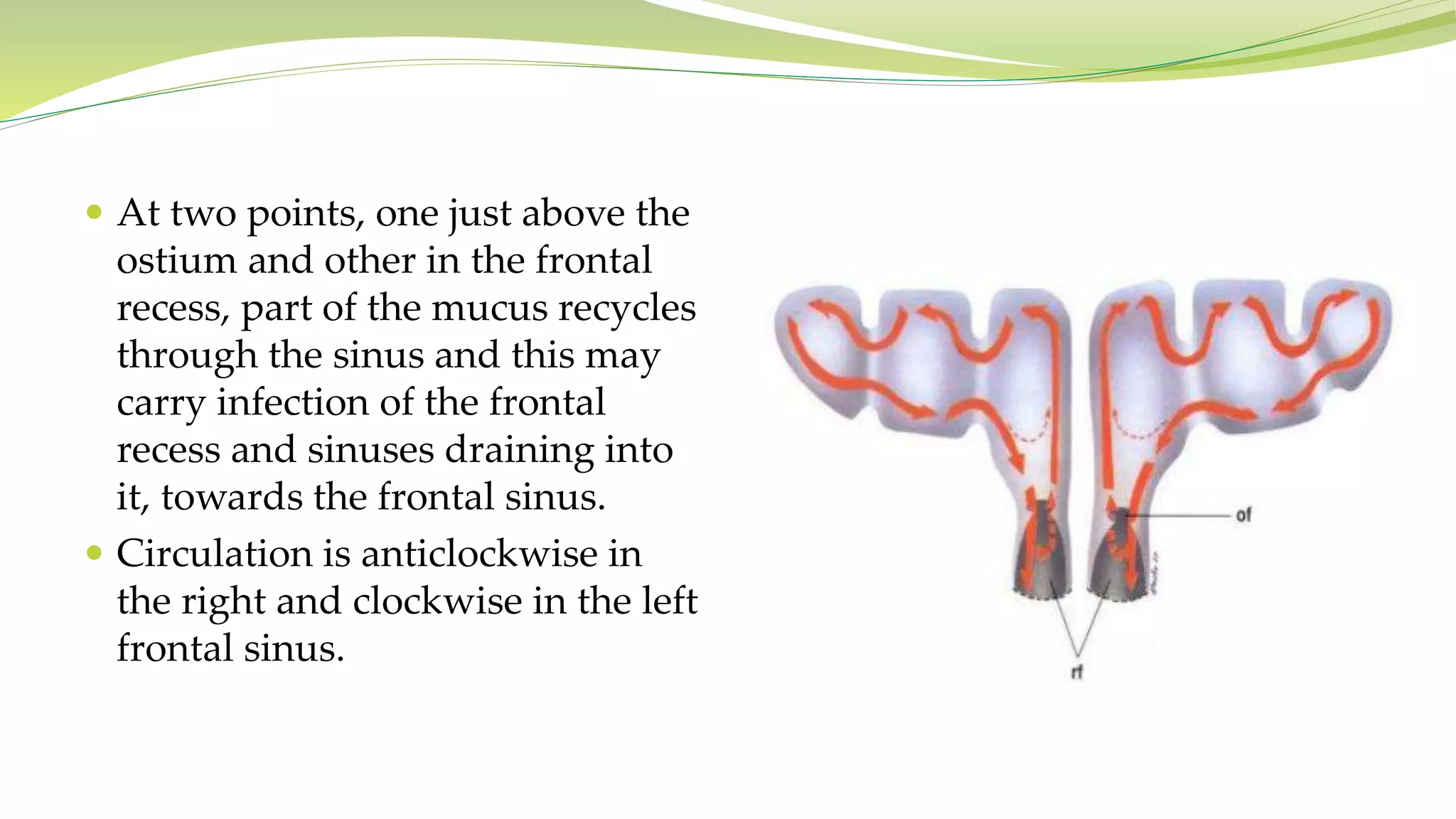
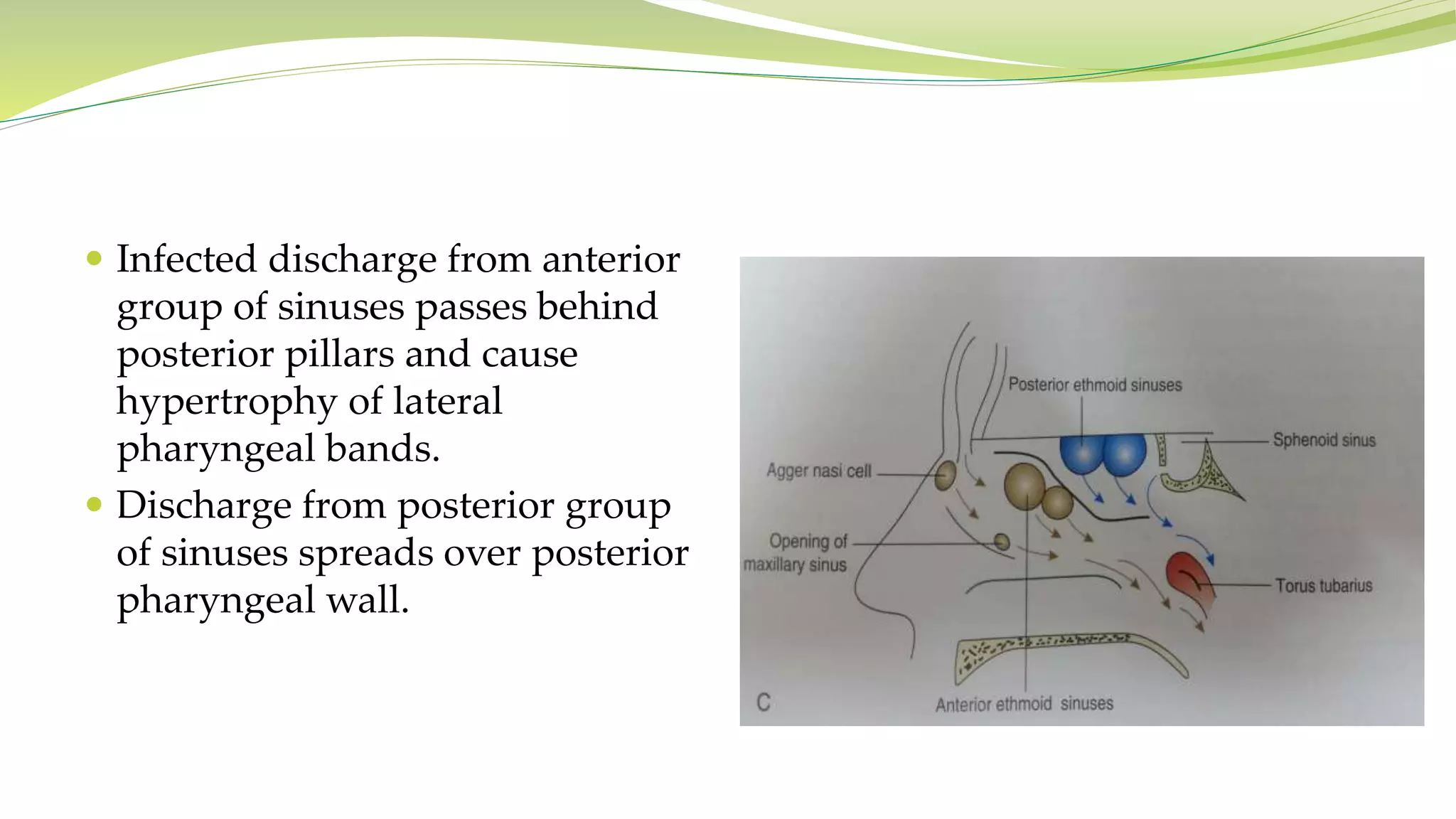
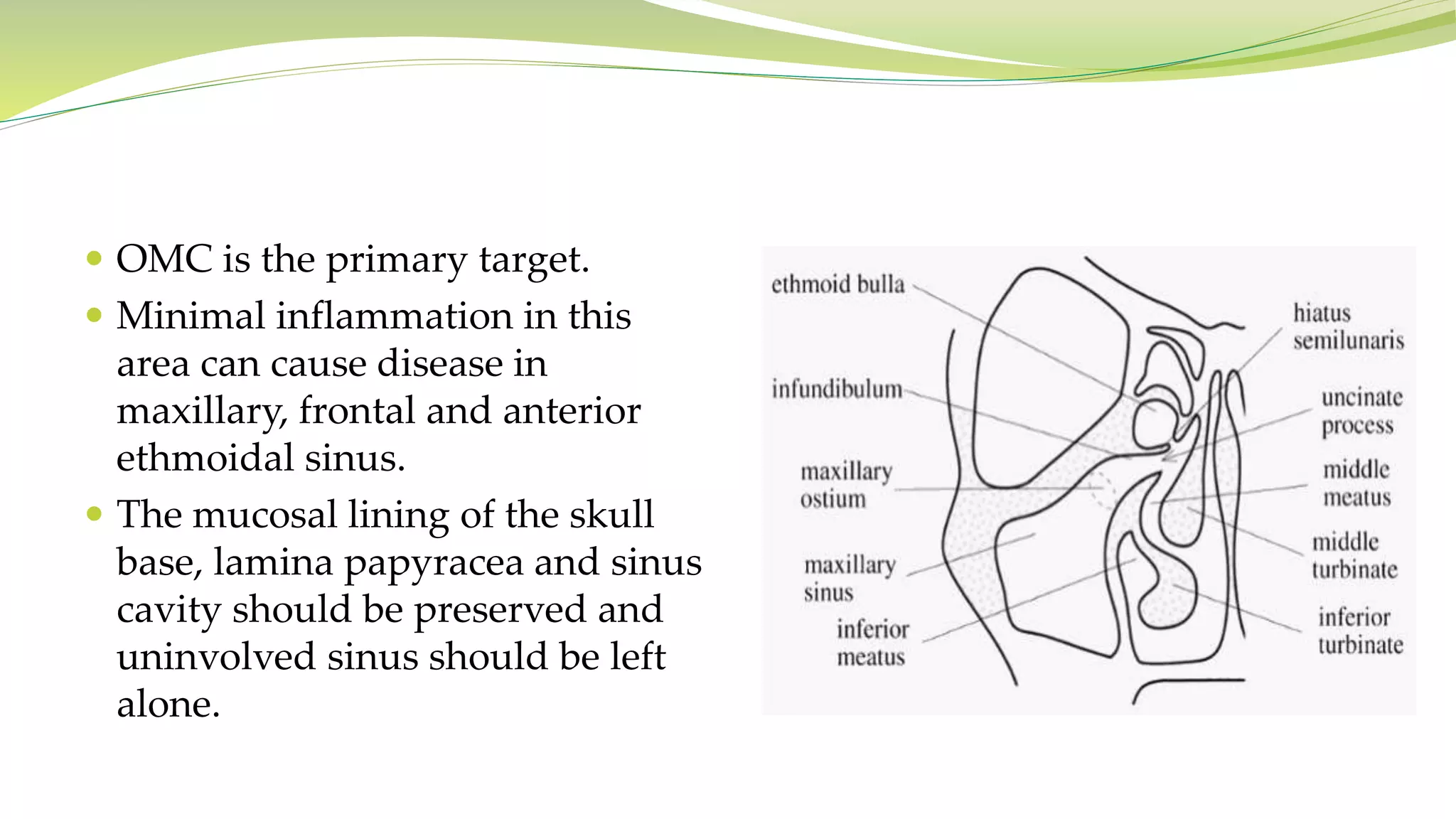

The document outlines the anatomy and function of paranasal sinuses, detailing their drainage mechanisms into the nasal cavity through mucociliary action. It discusses the mucous blanket's role in trapping pathogens and transporting mucus, emphasizing the significance of ciliary movement in sinus clearance. The principles of functional endoscopic sinus surgery (FESS) are also described, focusing on restoring ventilation and mucociliary function while preserving healthy tissue.





































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















