
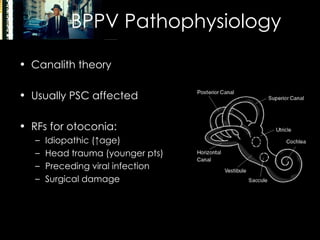
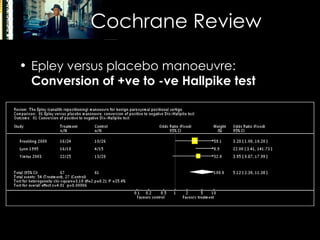
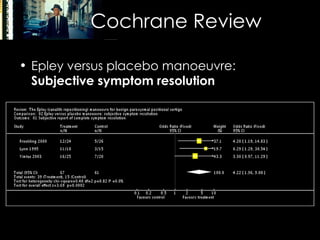

The document discusses vertigo, differentiating between central and peripheral causes, and highlights benign paroxysmal positional vertigo (BPPV) as a common source, with a focus on the Epley manoeuvre for treatment. It summarizes the pathophysiology, clinical features, and evidence supporting the effectiveness of the Epley manoeuvre, indicating that many patients may require multiple treatments. Key references and epidemiological insights are provided to support the information presented.


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








