Downloaded 16 times
![Compliance
• Compliance describes the
elasticity or distensibility of
the lungs & chest wall.
• Compliance = ΔV /ΔP
• ml/cmH2O
• Low Compliance means Stiff
lungs [as in RDS]. It will
need higher pressure
gradient for pushing air
inside.](https://image.slidesharecdn.com/basicsofmechanicalventilatordrasaduzzaman-230716123538-2d0fb71f/75/basics-of-mechanical-ventilator-Dr-Asaduzzaman-pptx-14-2048.jpg)
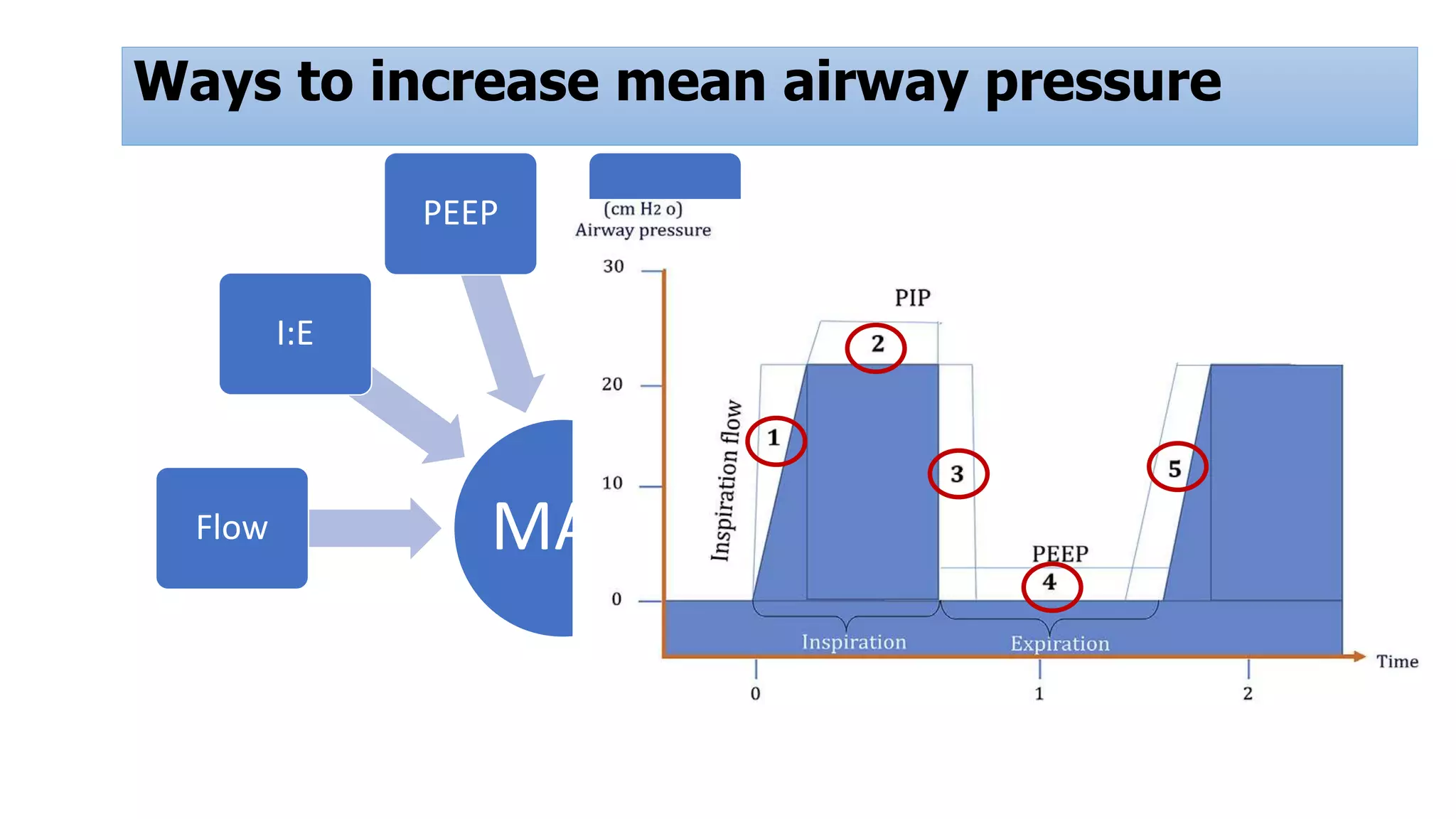

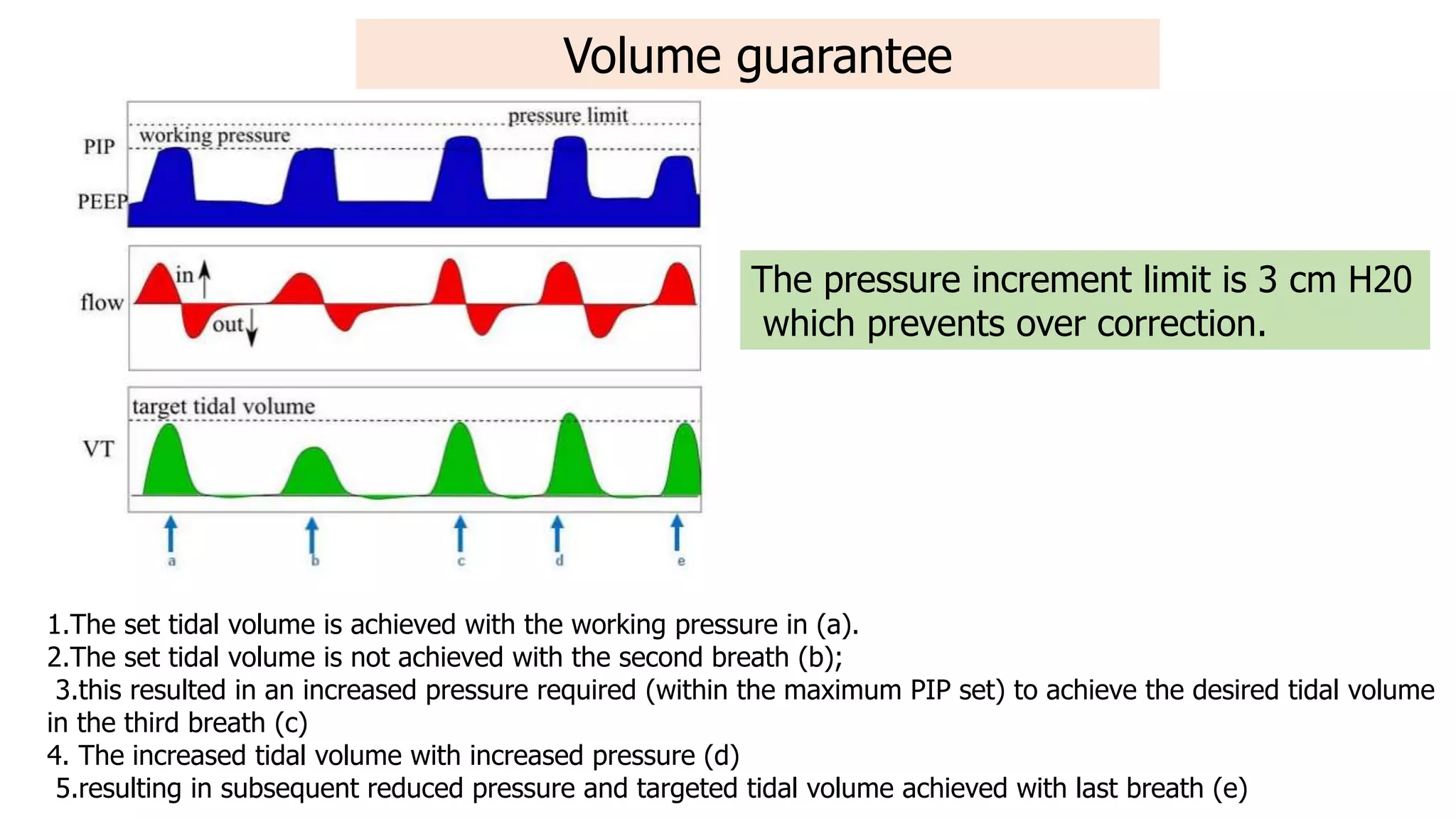
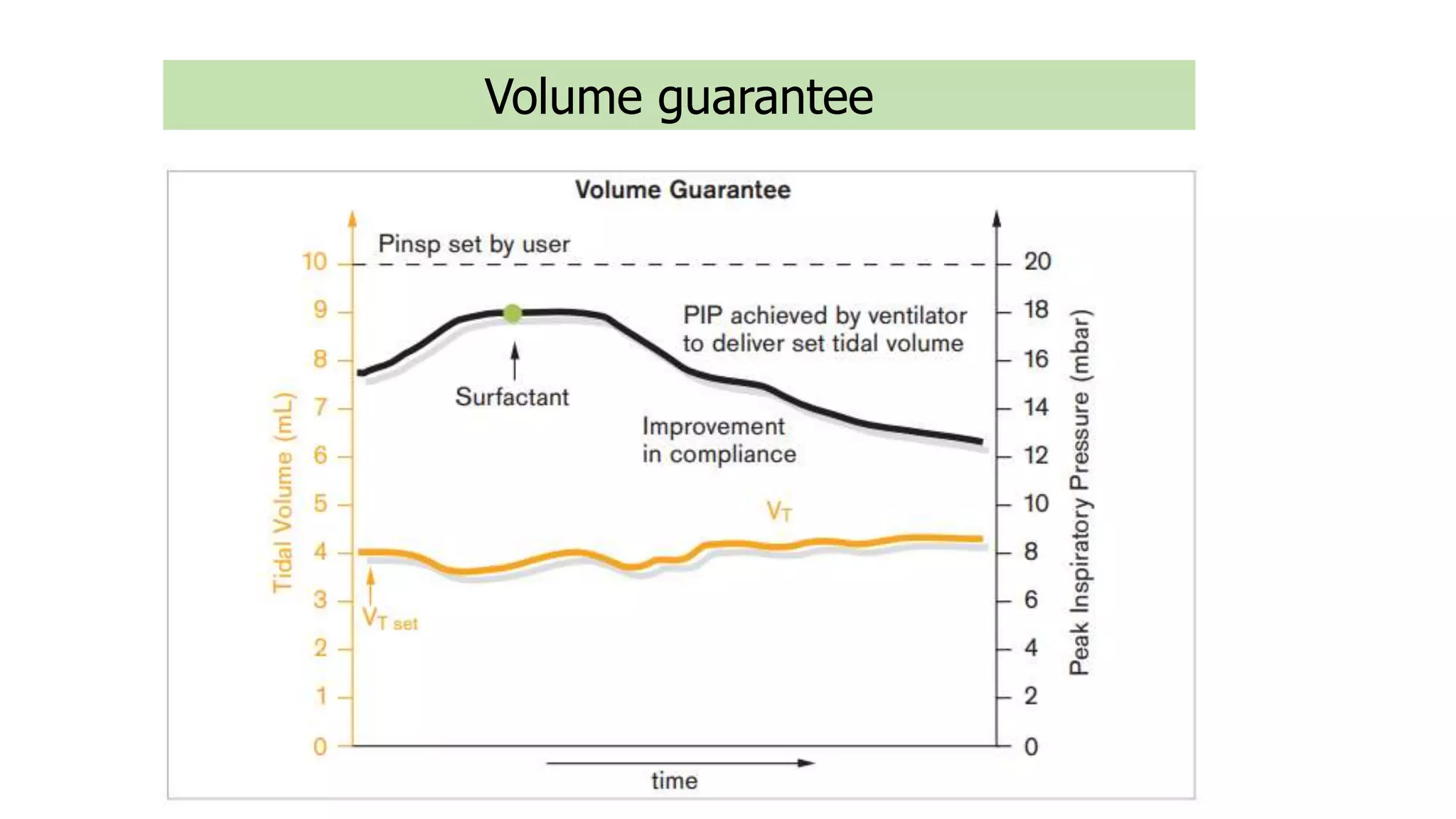




Mechanical ventilation is an important life-saving intervention for extremely premature and sick newborns. While it supports oxygenation and carbon dioxide removal, it can also cause lung injury if not optimized. The document discusses the physiology of ventilation, components of mechanical ventilators like pressures and volumes, basic ventilation modes, and pulmonary graphics. Modes like volume guarantee aim to balance supporting gas exchange while limiting volumes and pressures. Understanding ventilation principles, ventilator operations, and individualizing strategies are important for achieving optimal outcomes for mechanically ventilated newborns.
Introduction to mechanical ventilation and its importance for sick neonates. 75% of infants are ventilated within 3 days. However, survival rate is low: 18%.
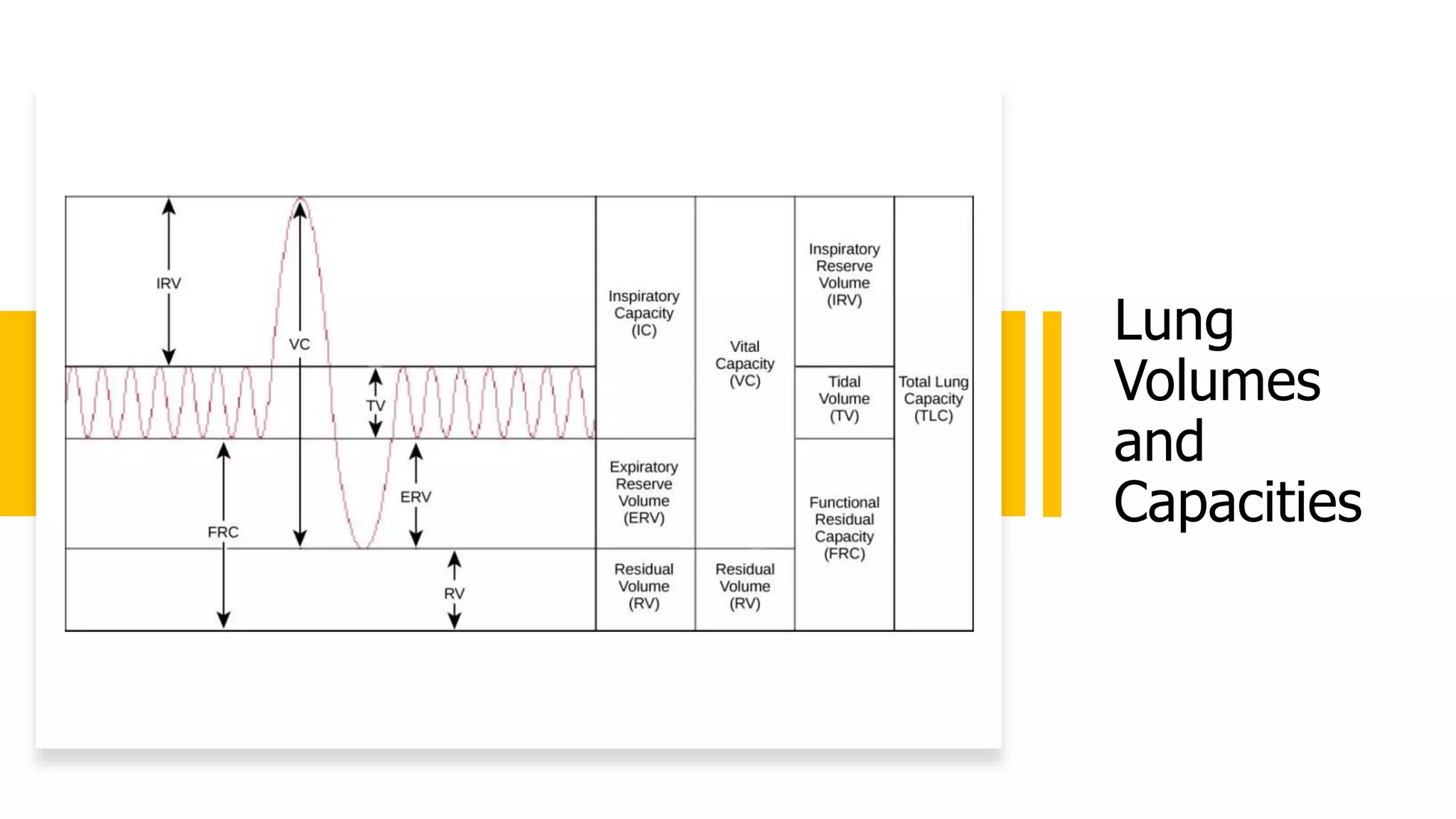
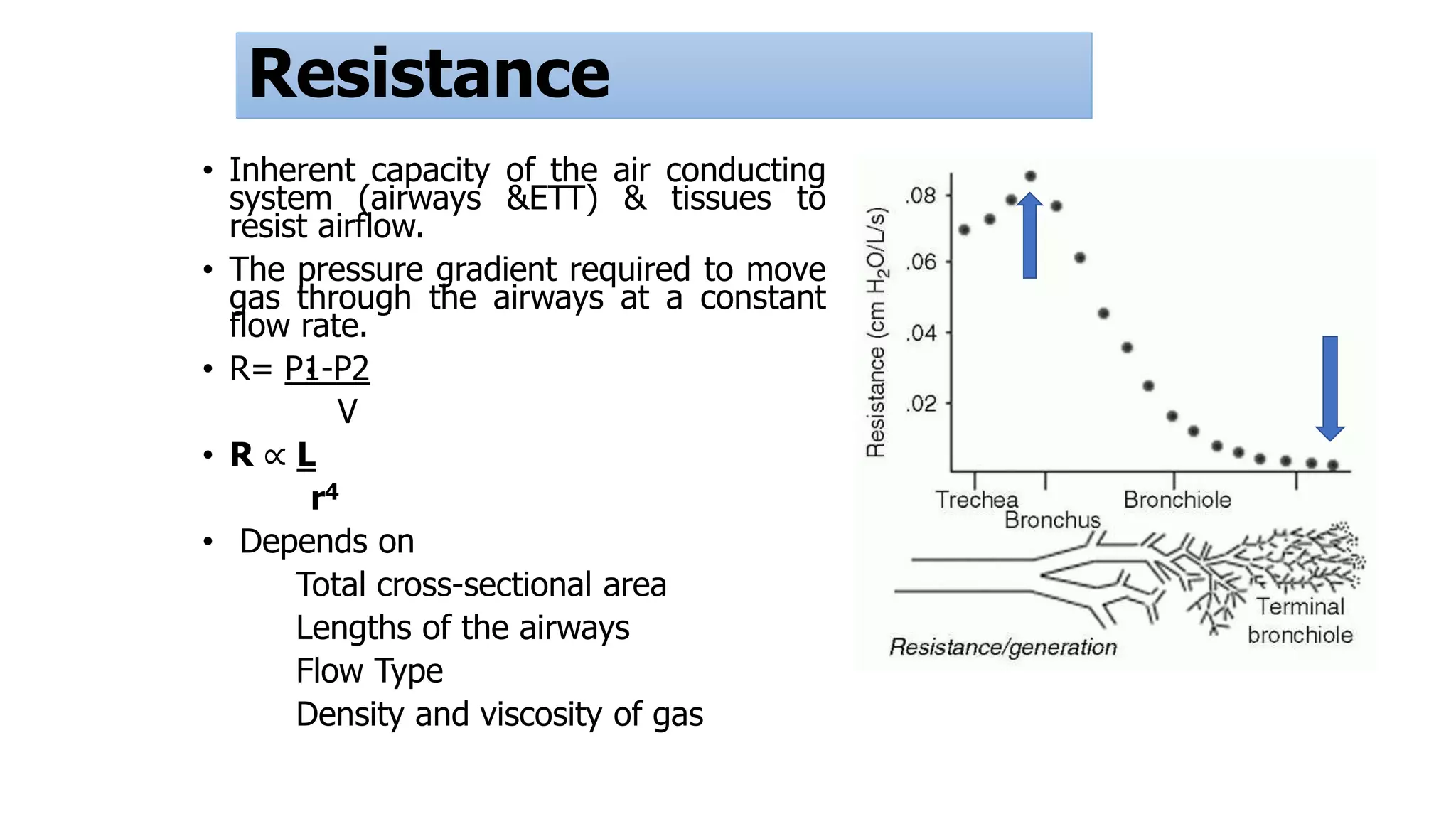
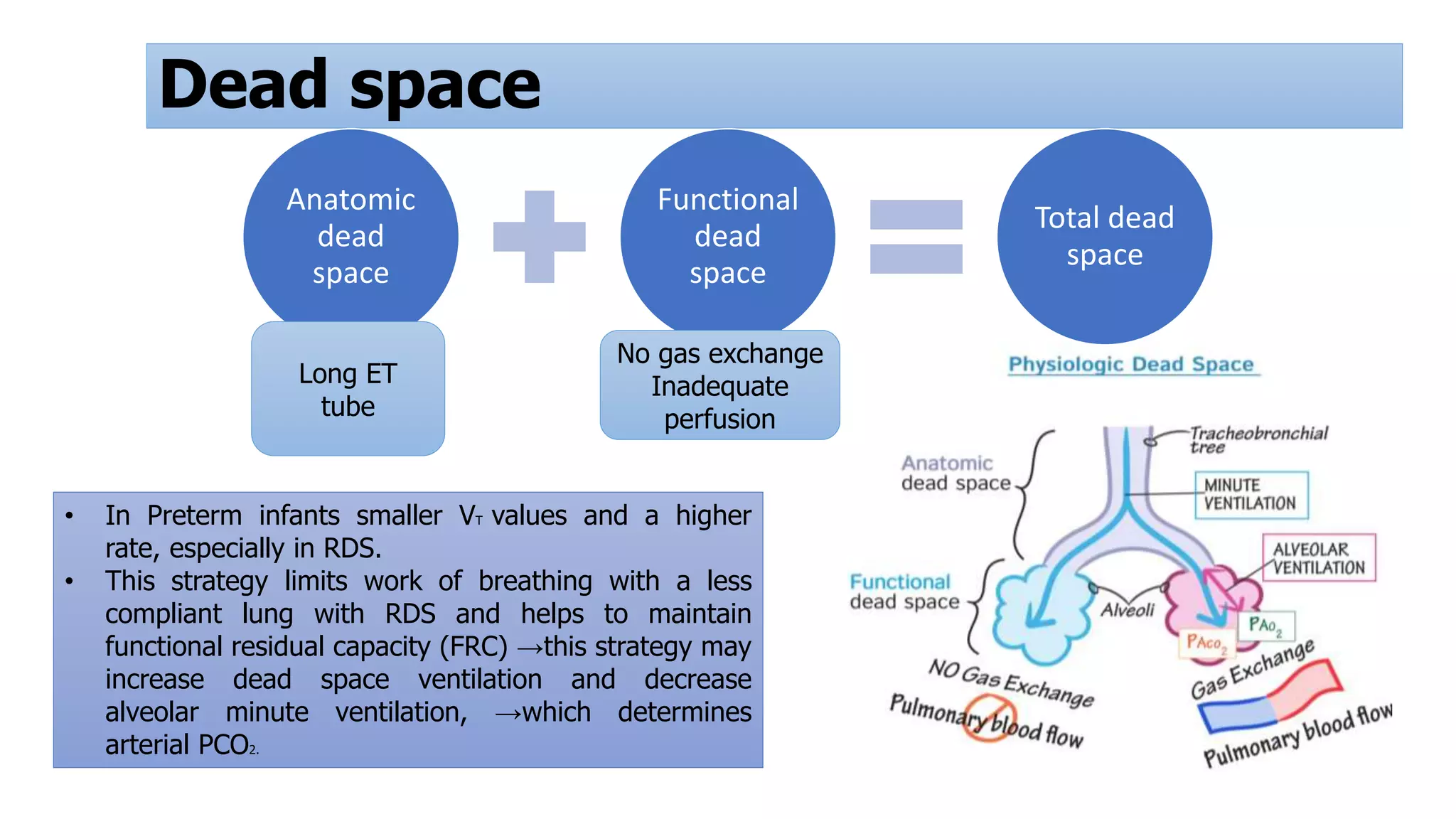
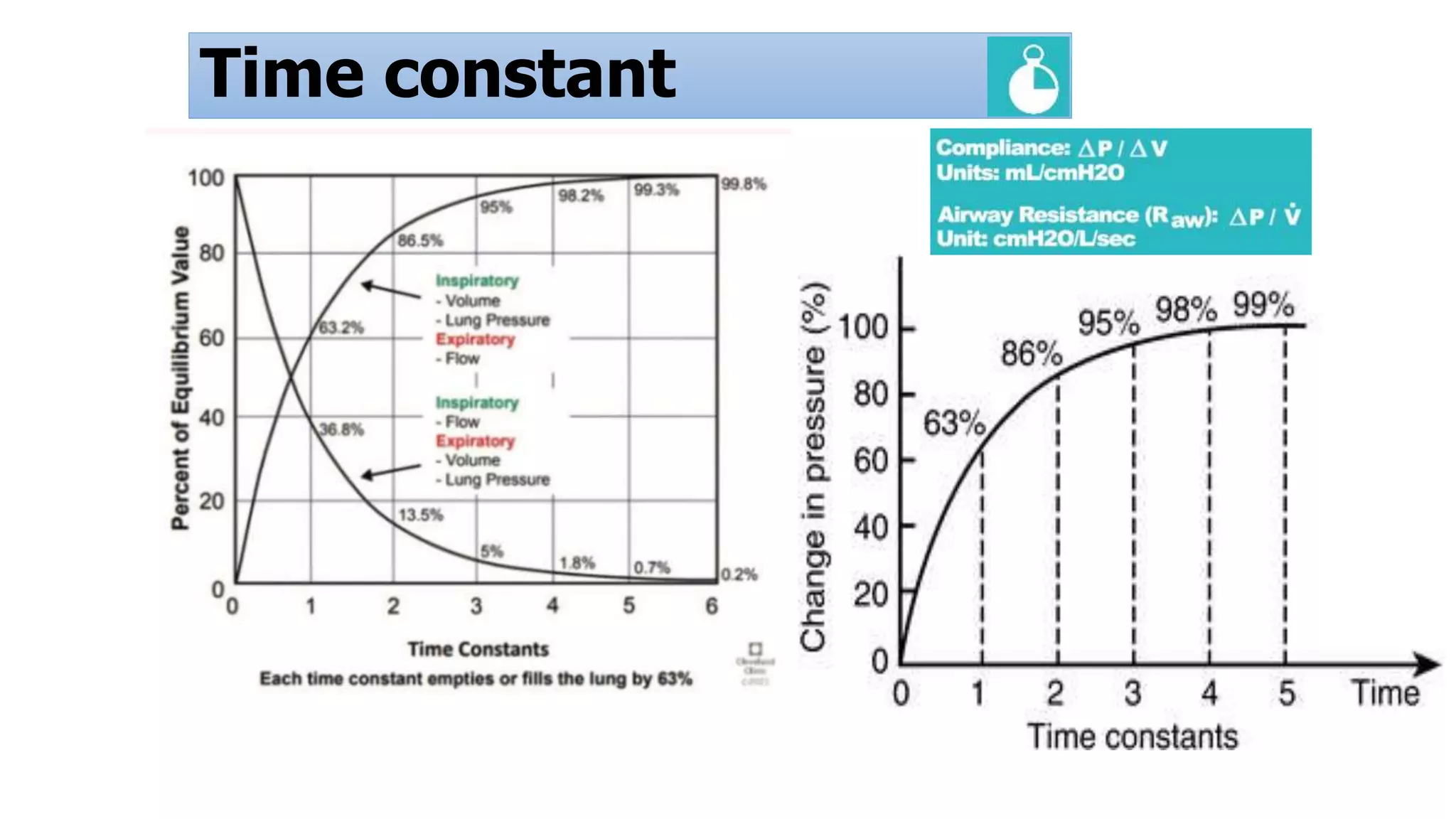
Understanding respiratory physiology and ventilator principles is crucial. Compliance, resistance, and dead space are important factors affecting ventilation.
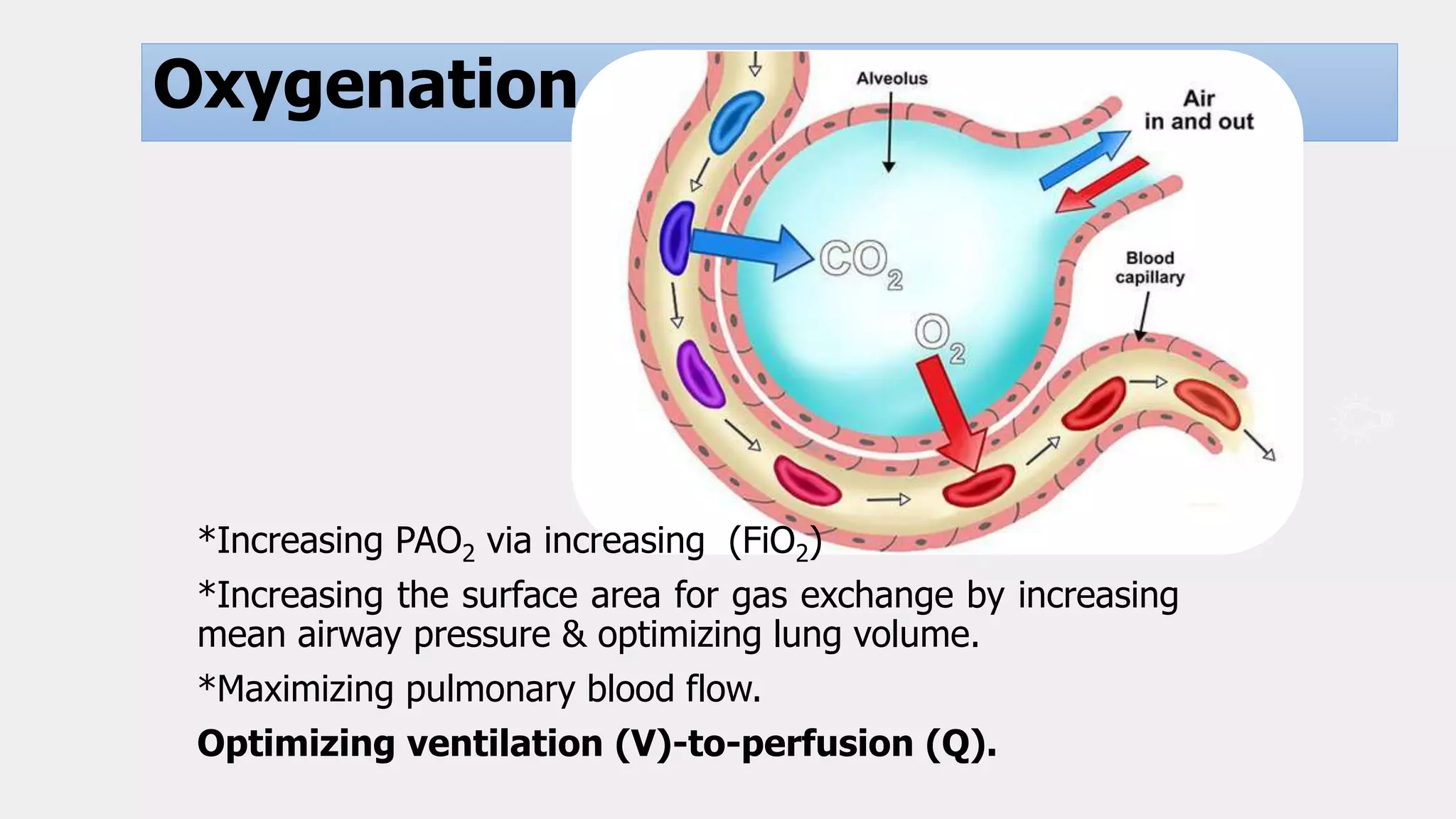
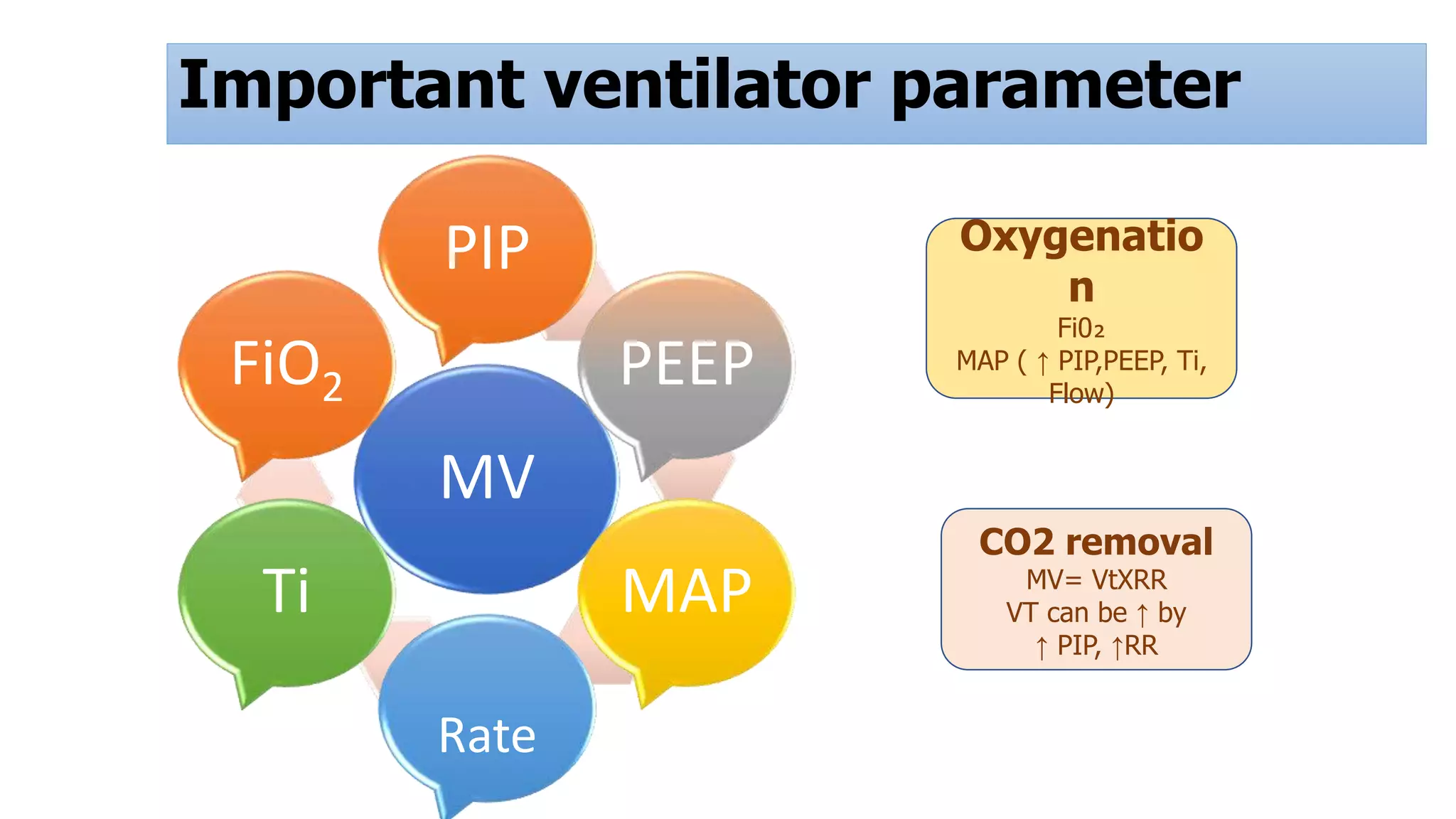
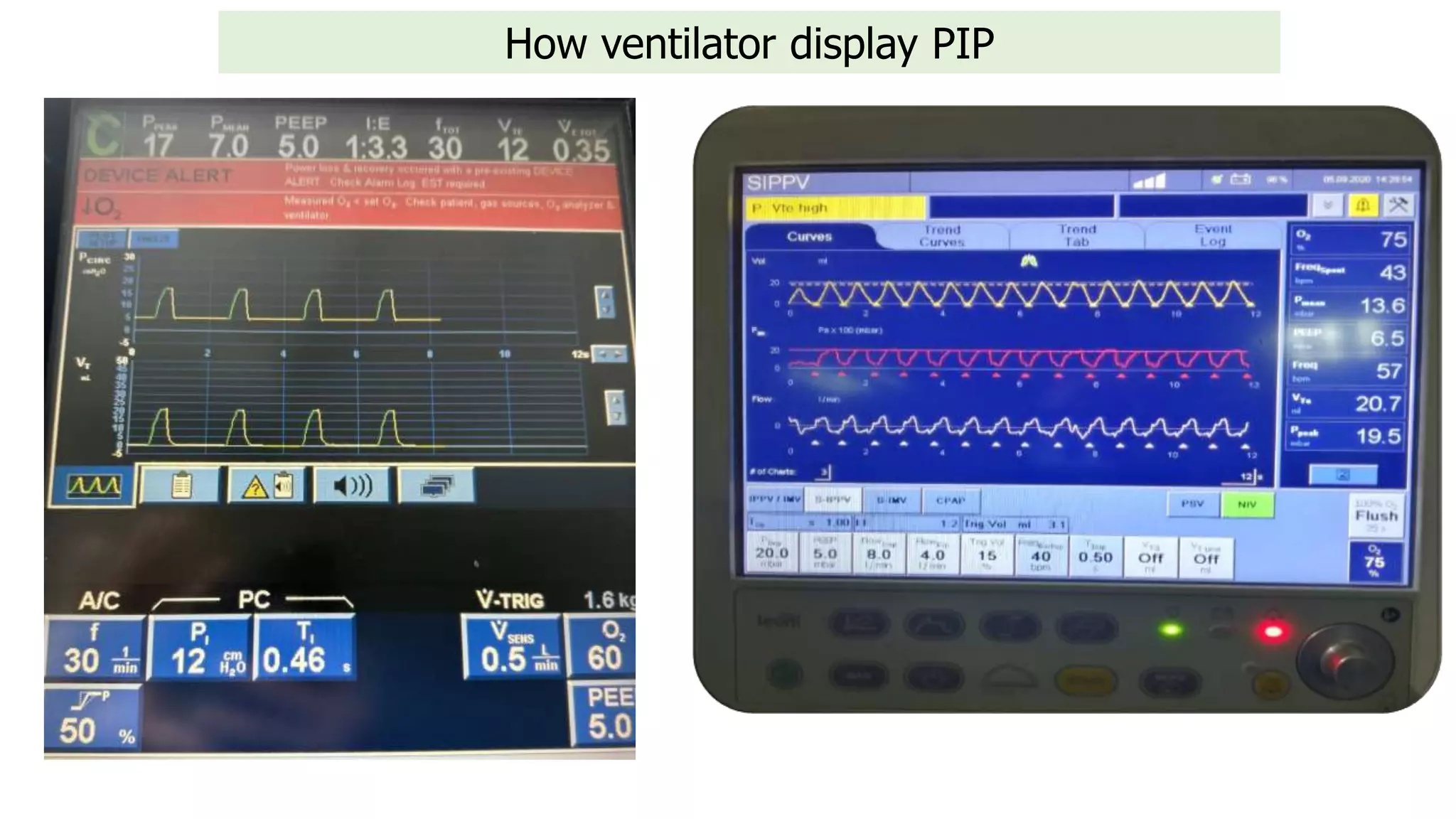
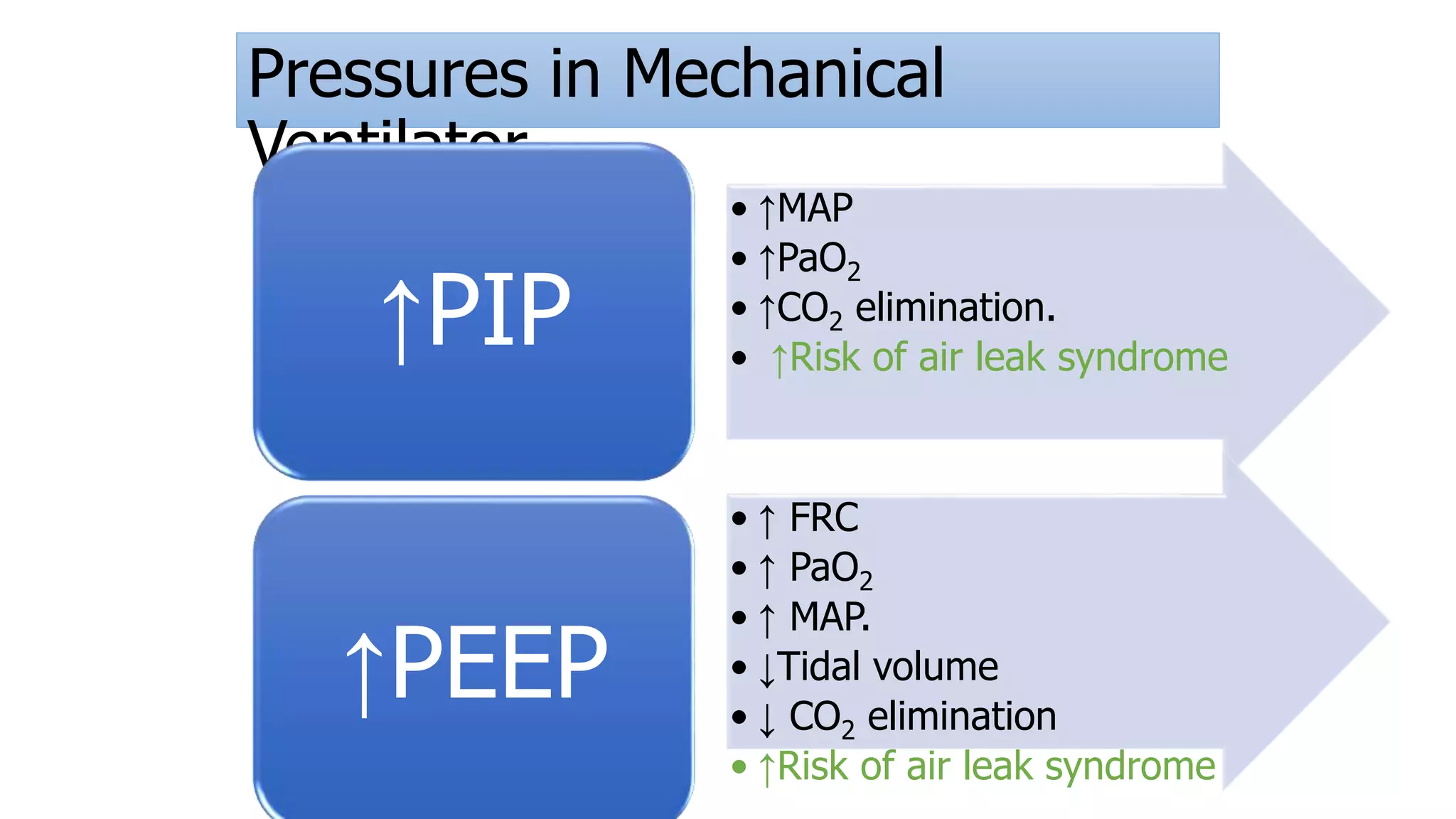
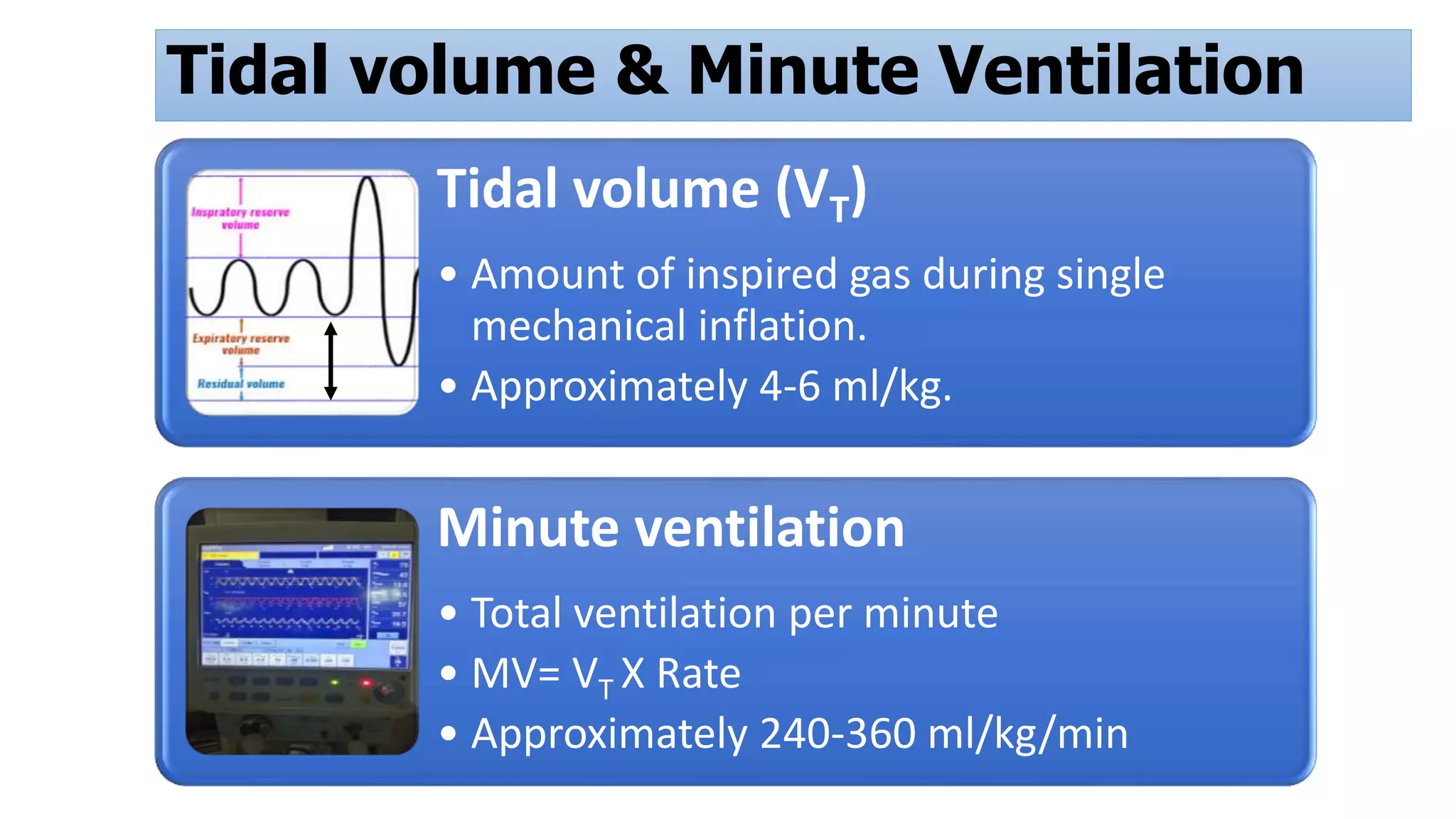
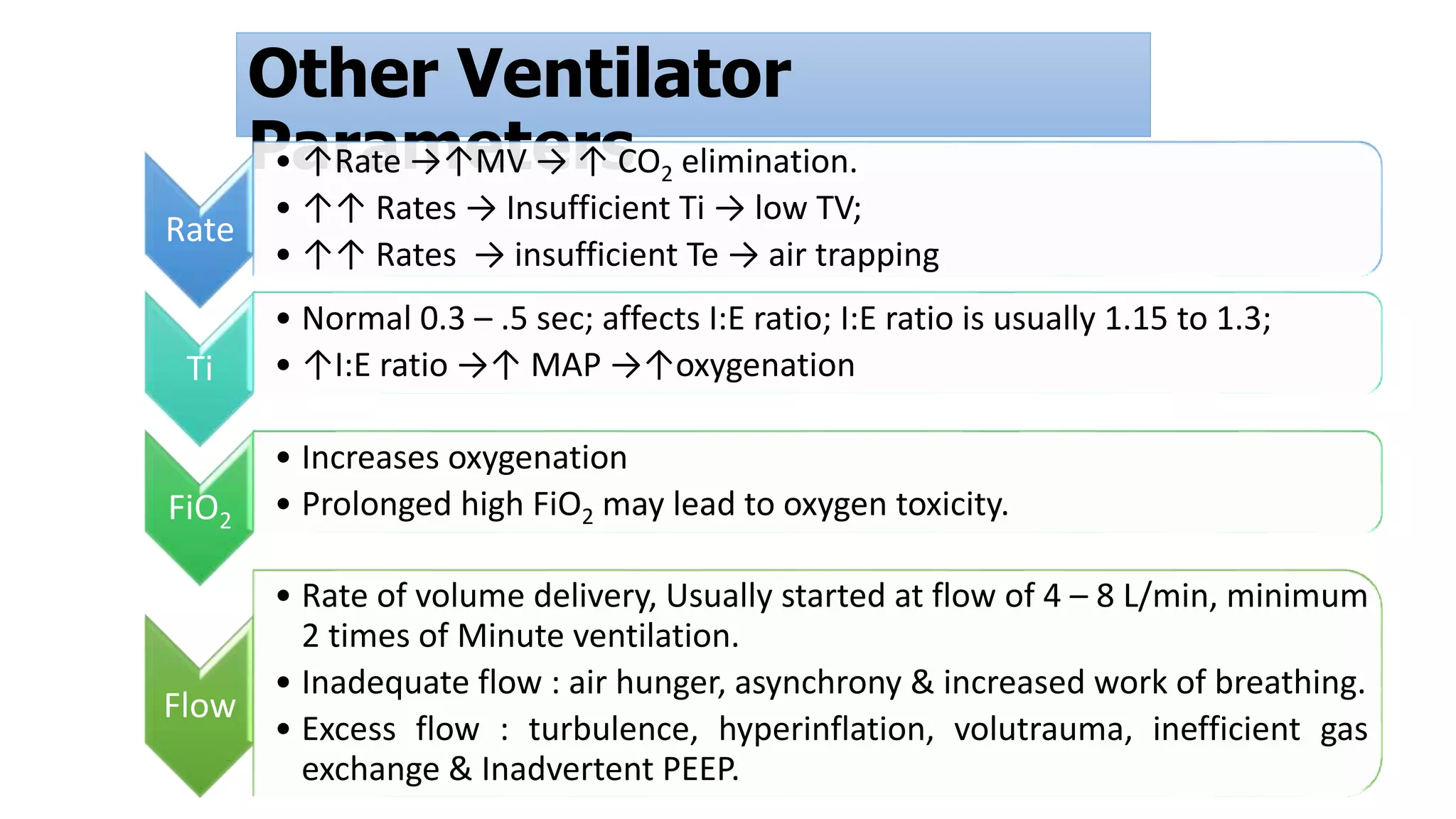
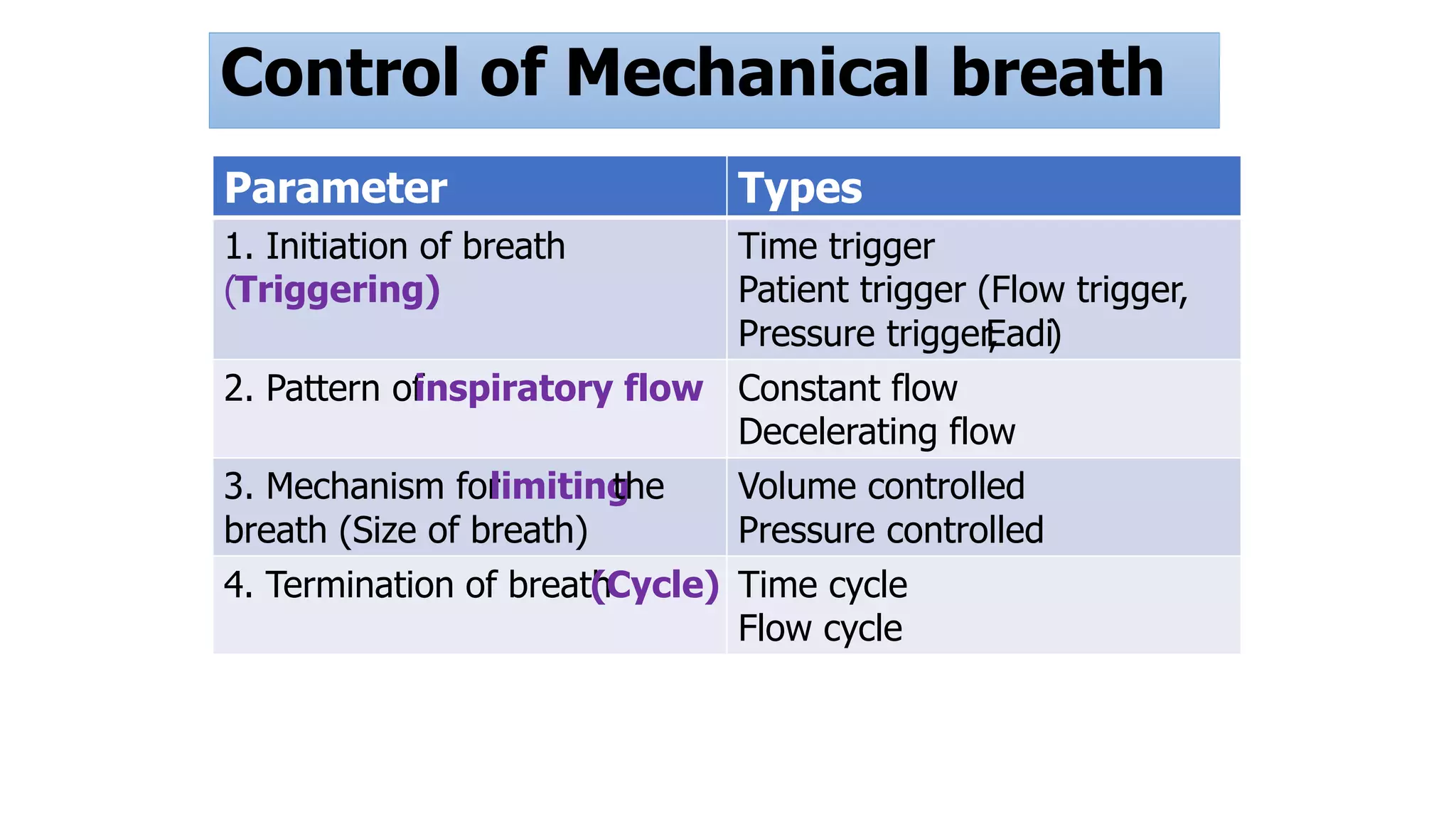
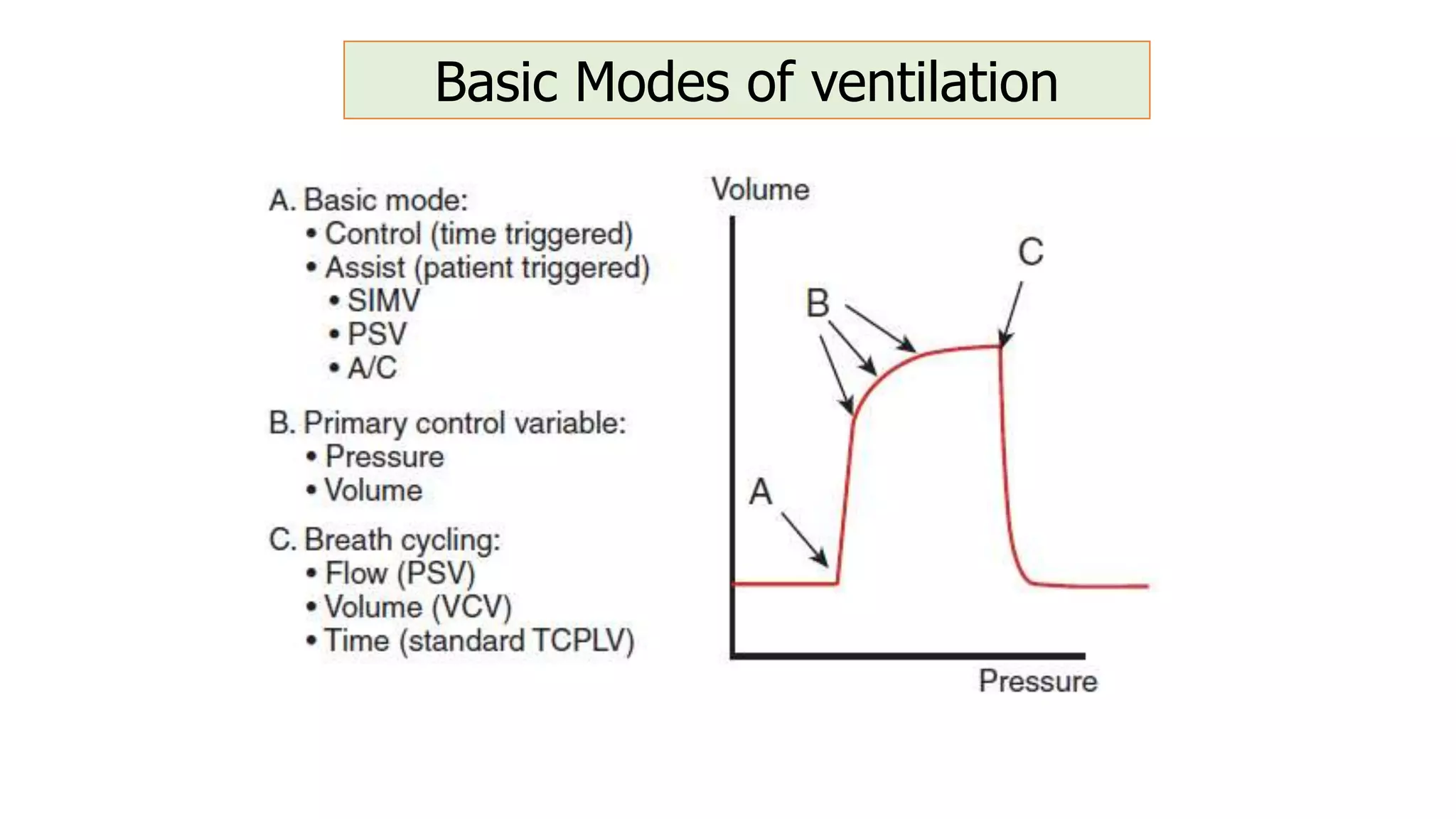
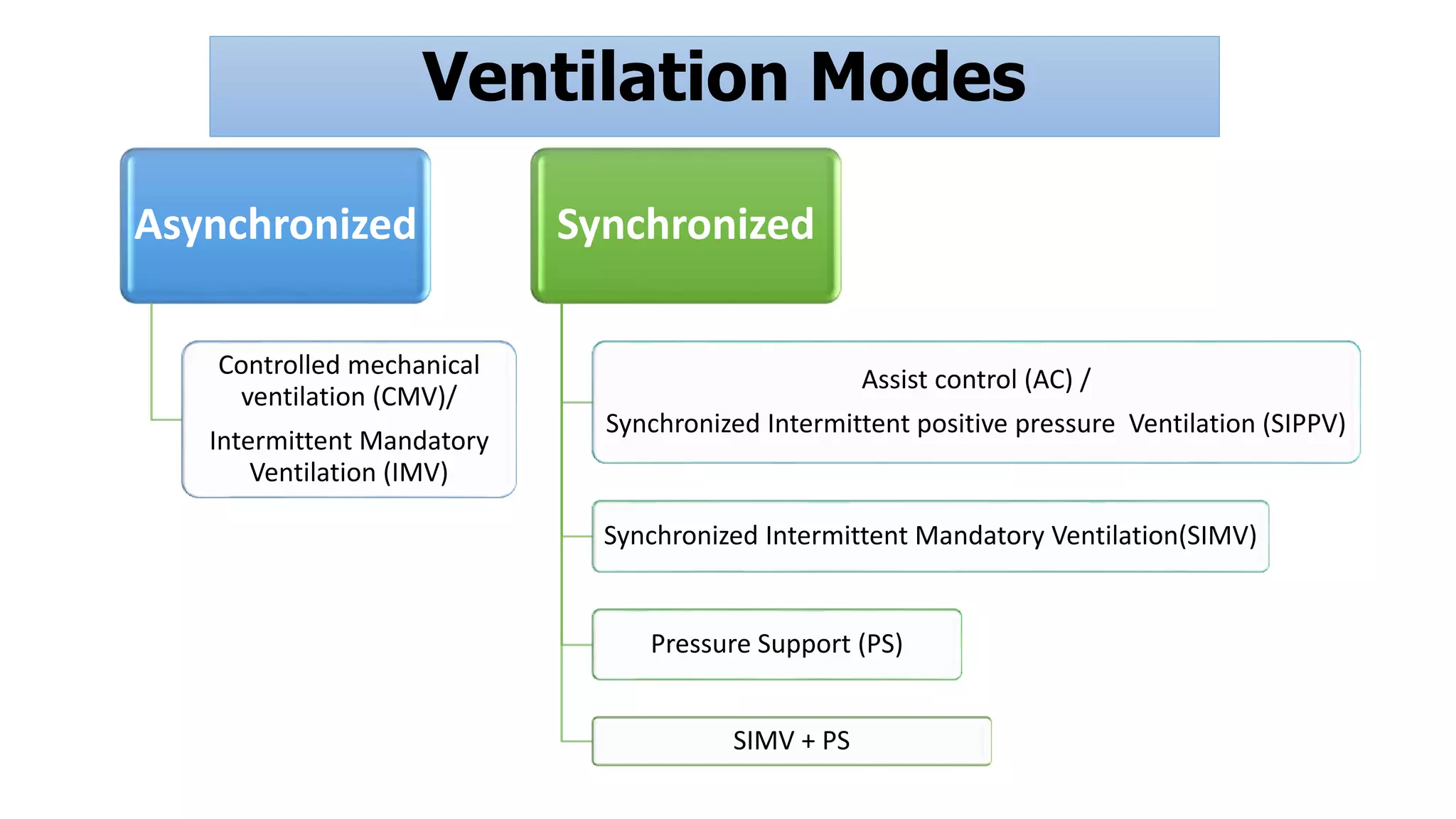
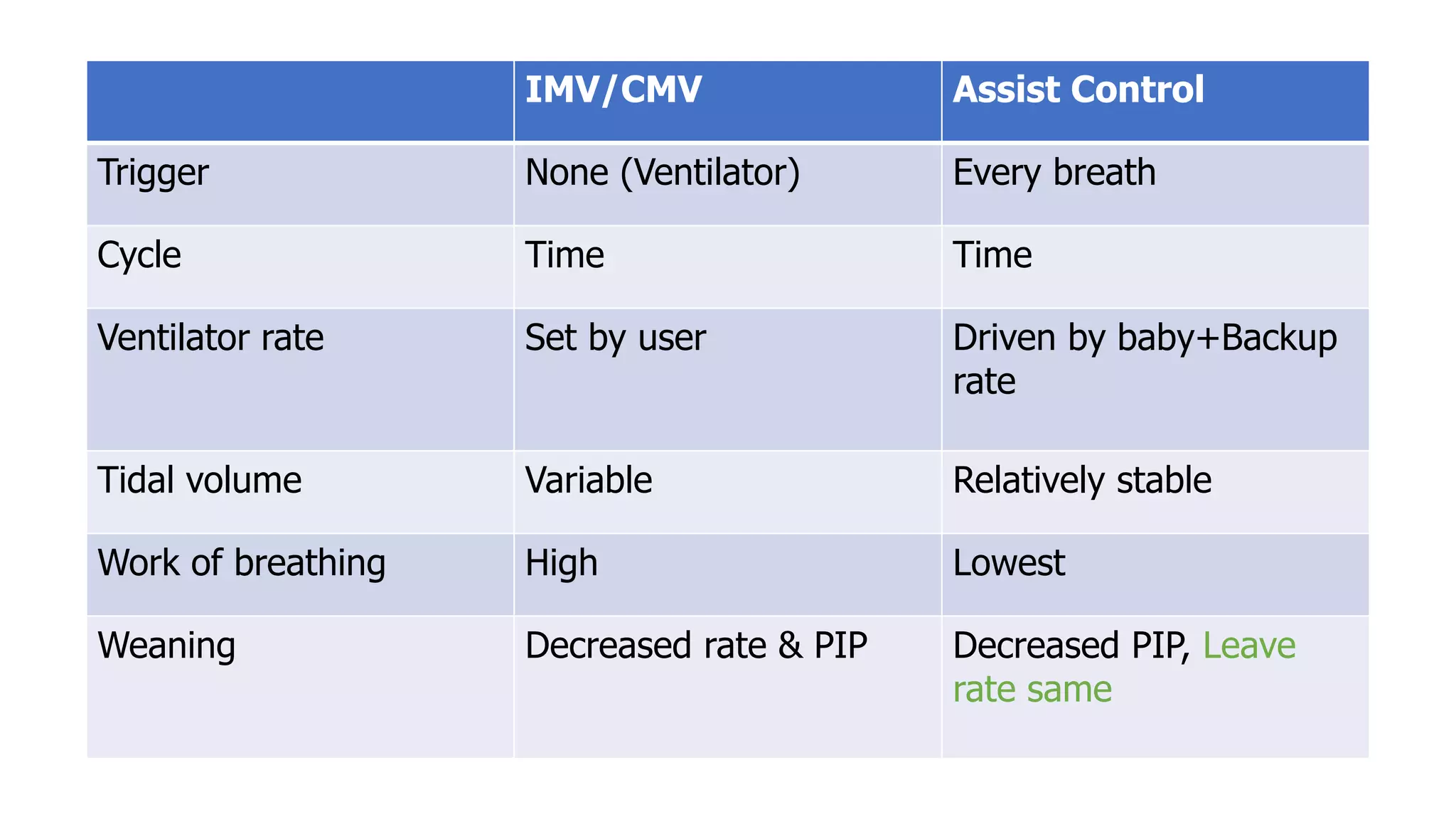
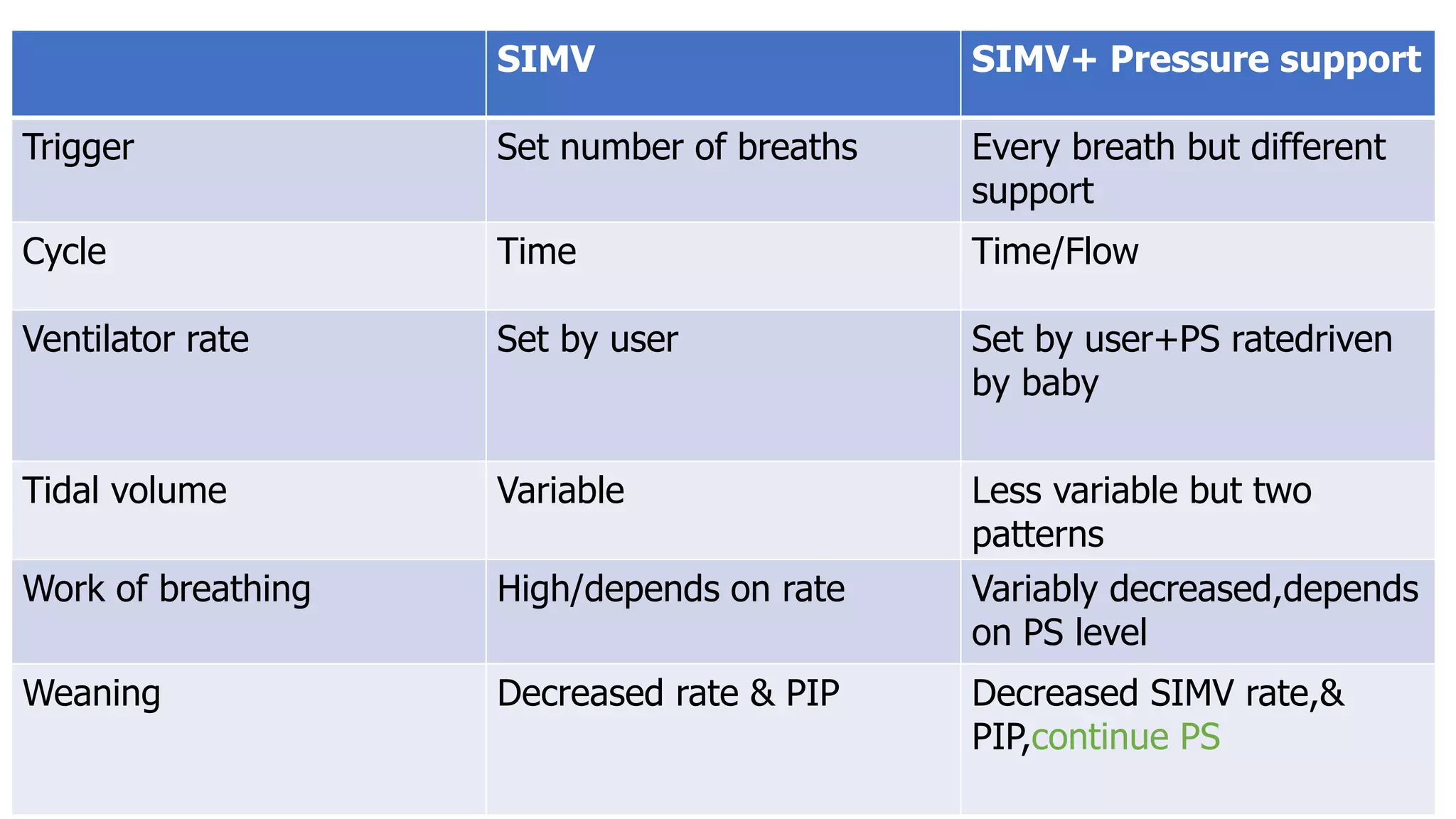
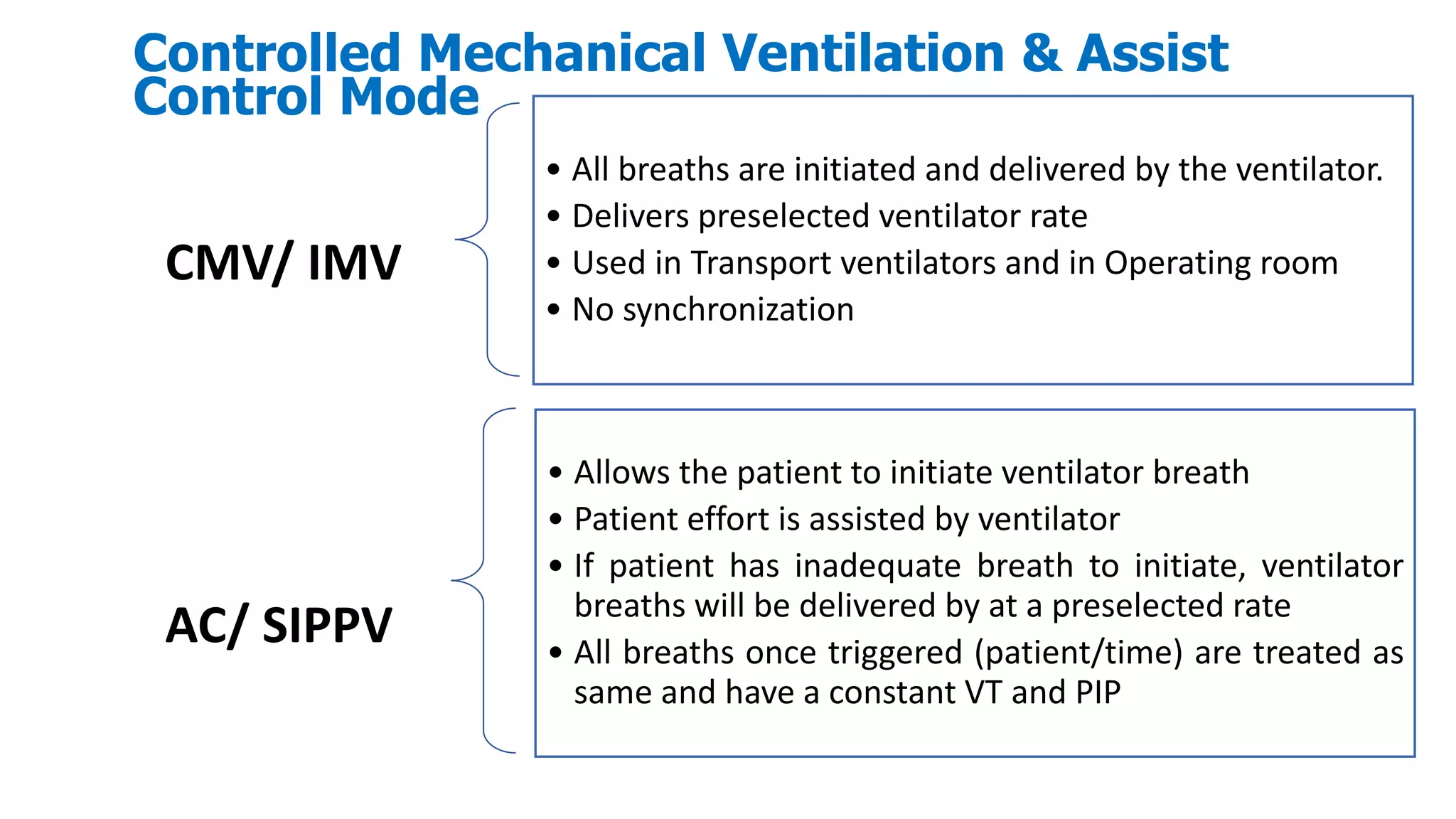
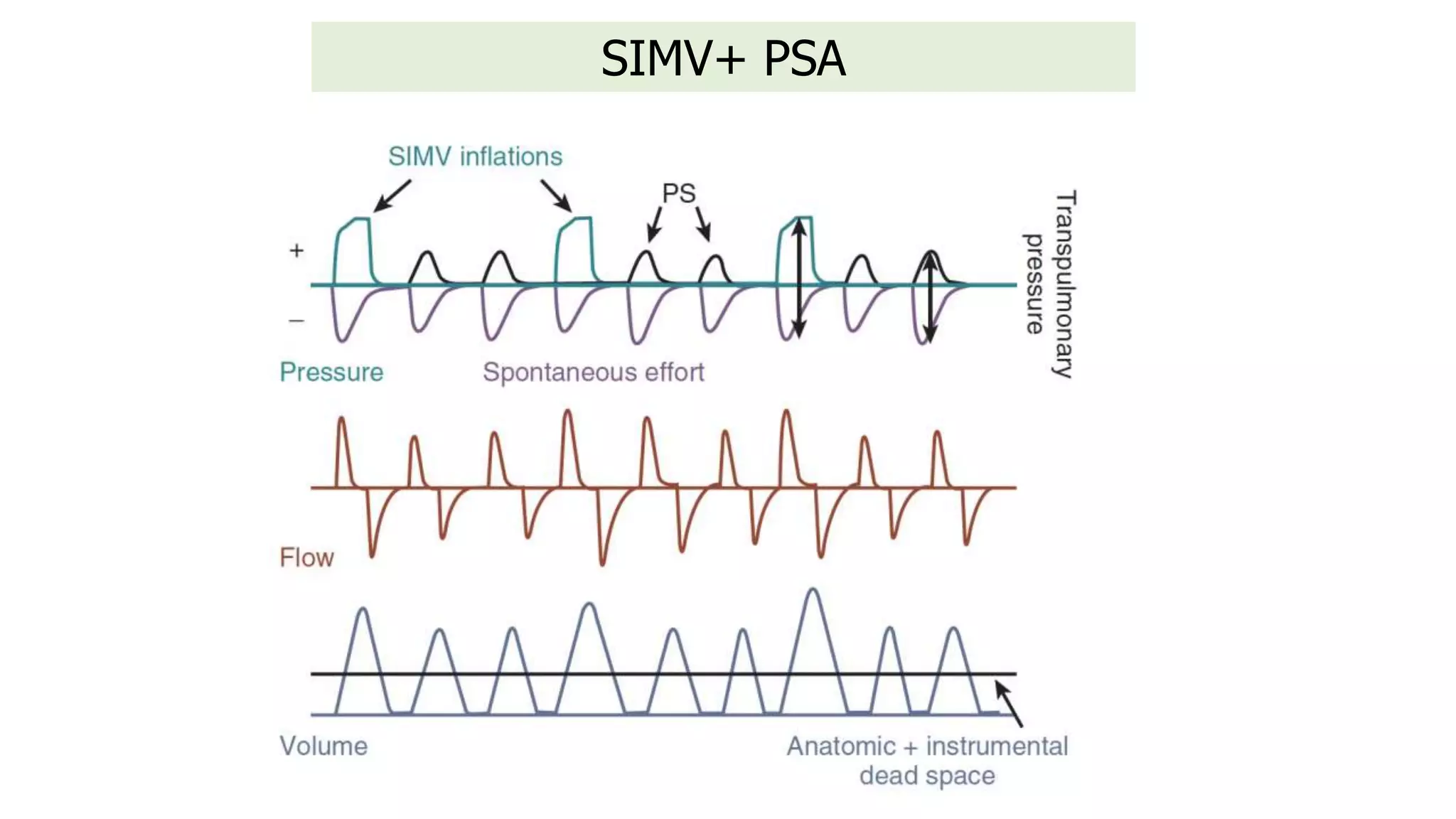
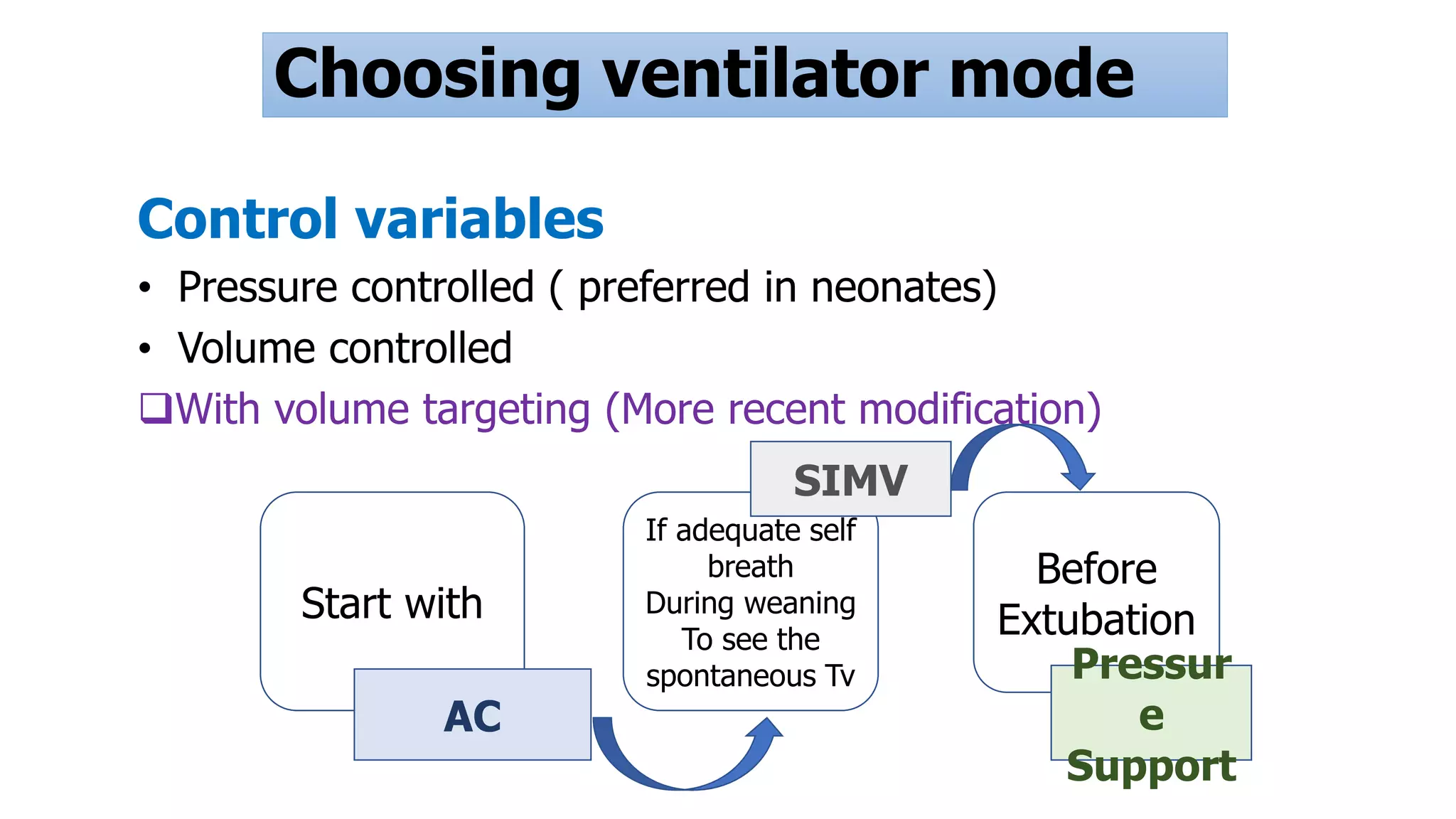
Key concepts of mechanical ventilation include lung volume, oxygenation support, and CO2 removal. Various ventilation modes (e.g., CMV, SIMV), important parameters like PIP, MAP, and tidal volume.
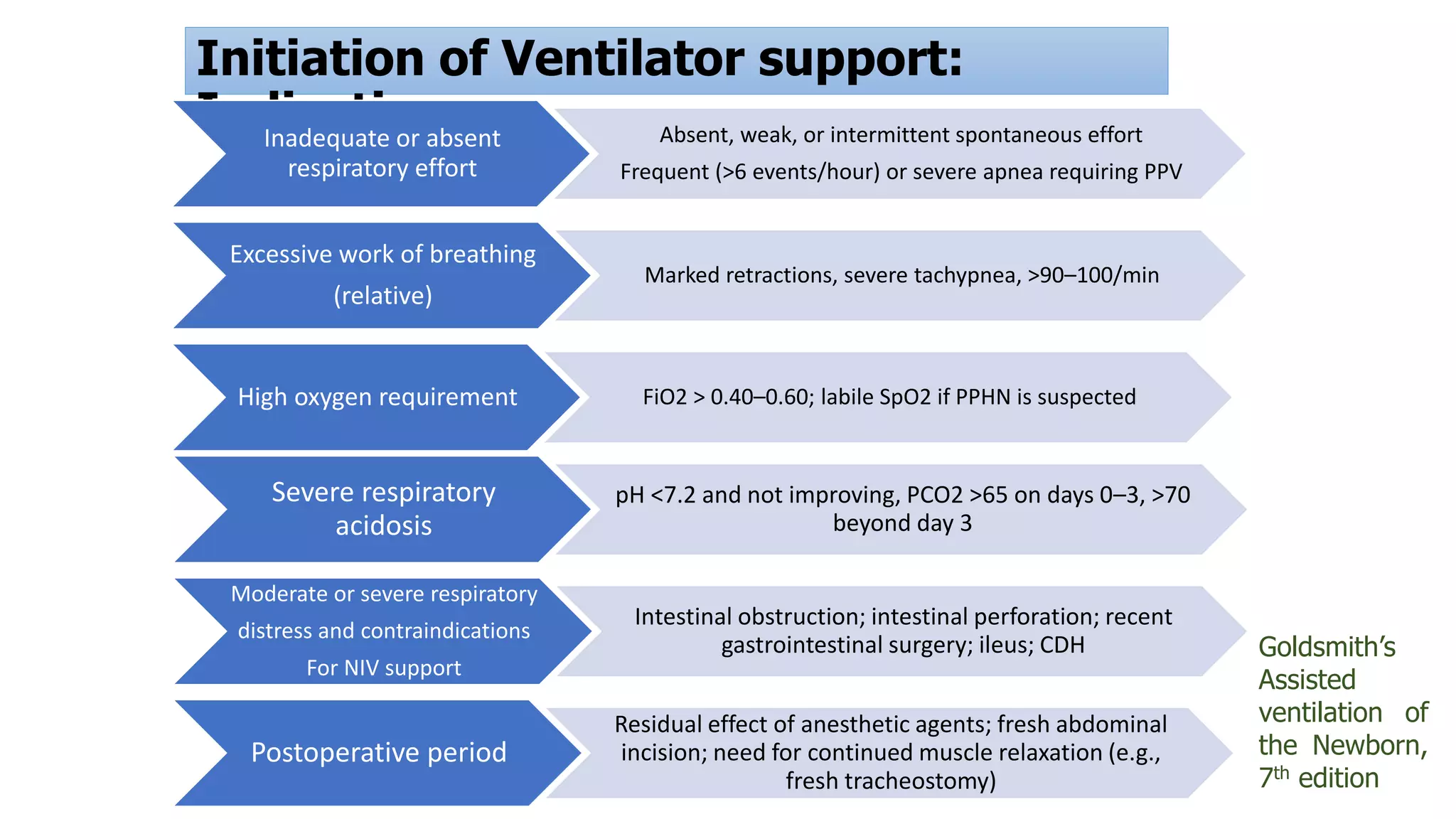
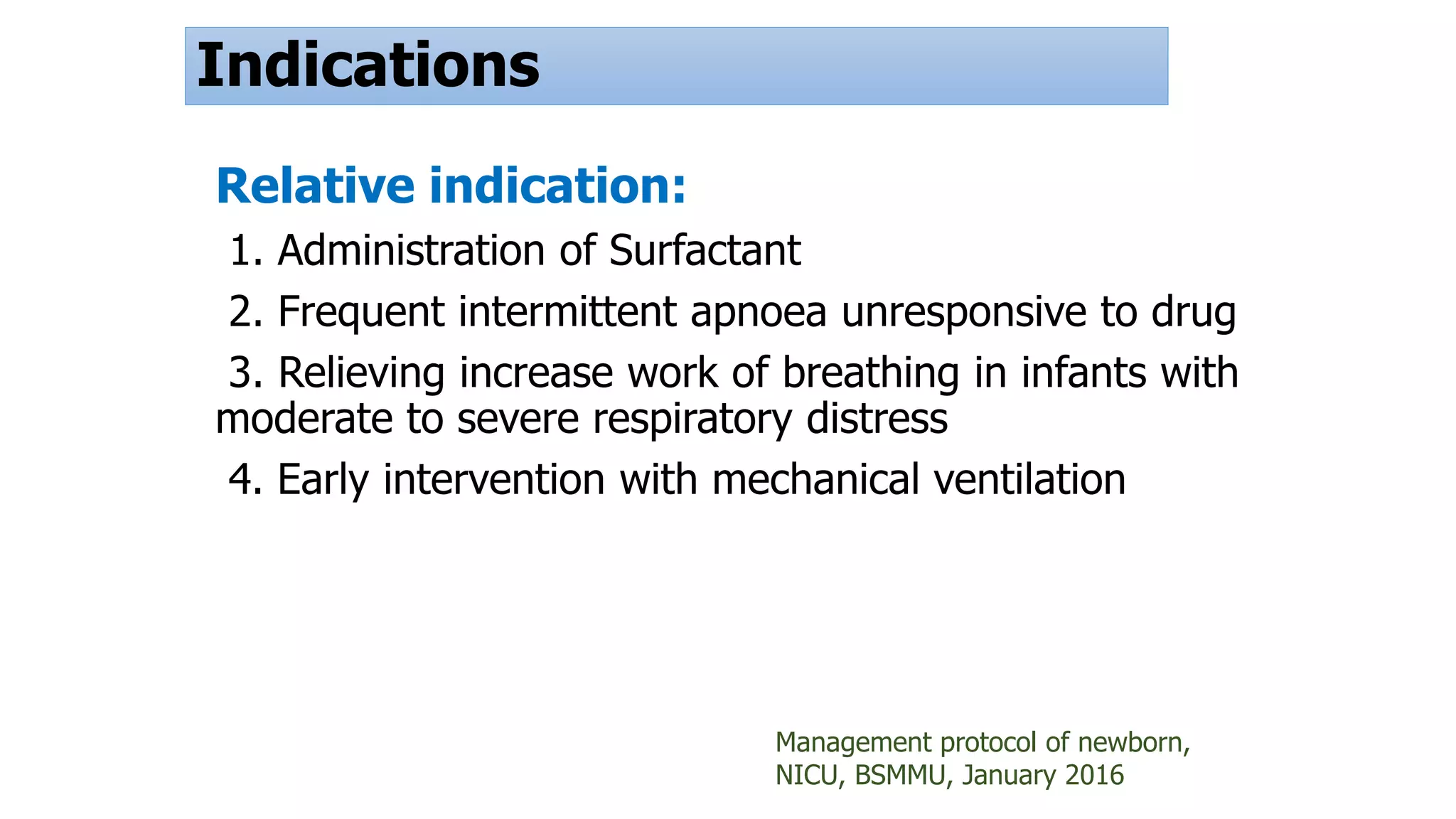
Indications include inadequate respiratory effort, severe apnea, and high oxygen needs. Relative indications discussed.Selecting ventilator modes, volume targeting benefits, and outcomes in terms of reduced death rates and complications.
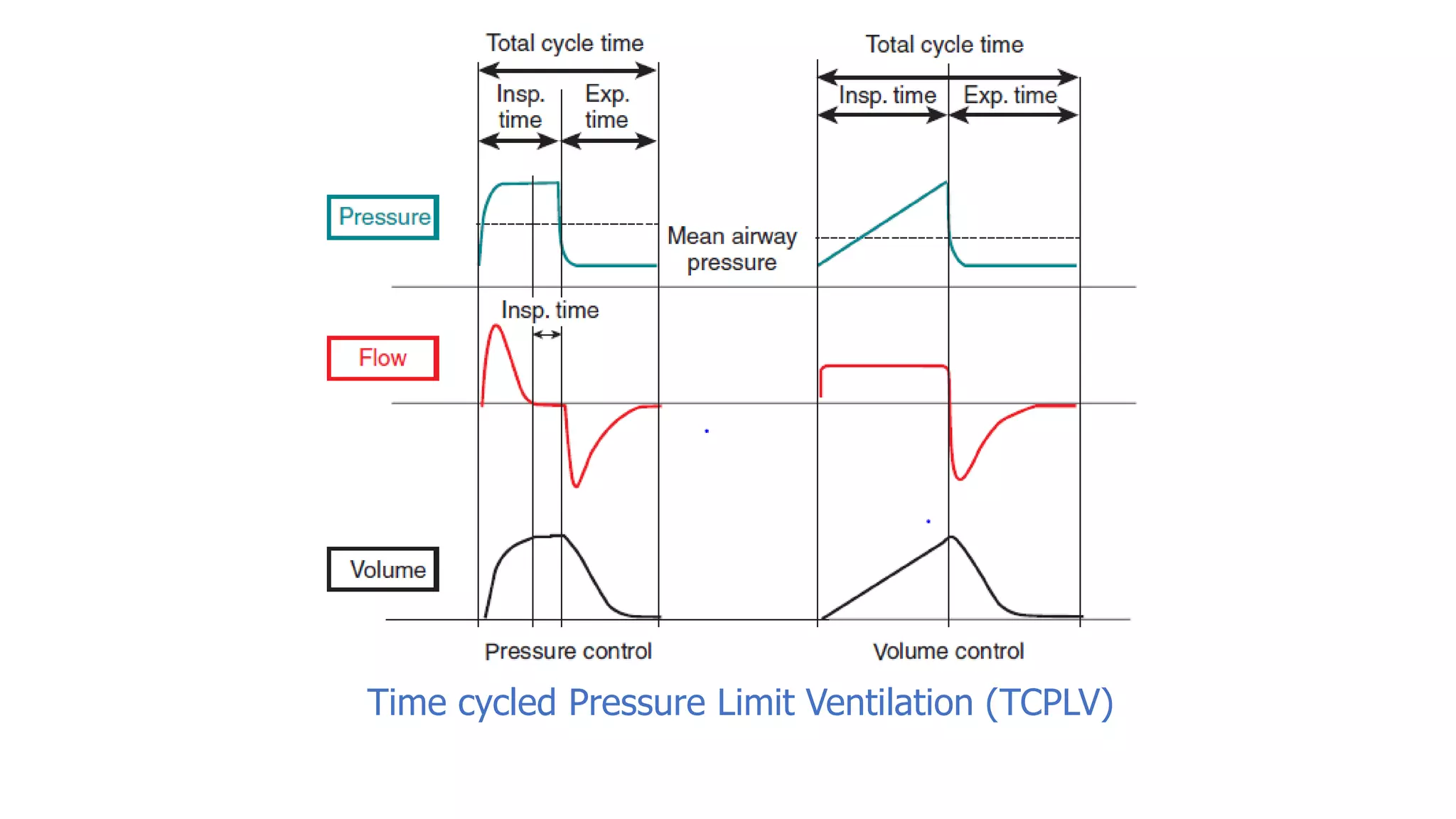
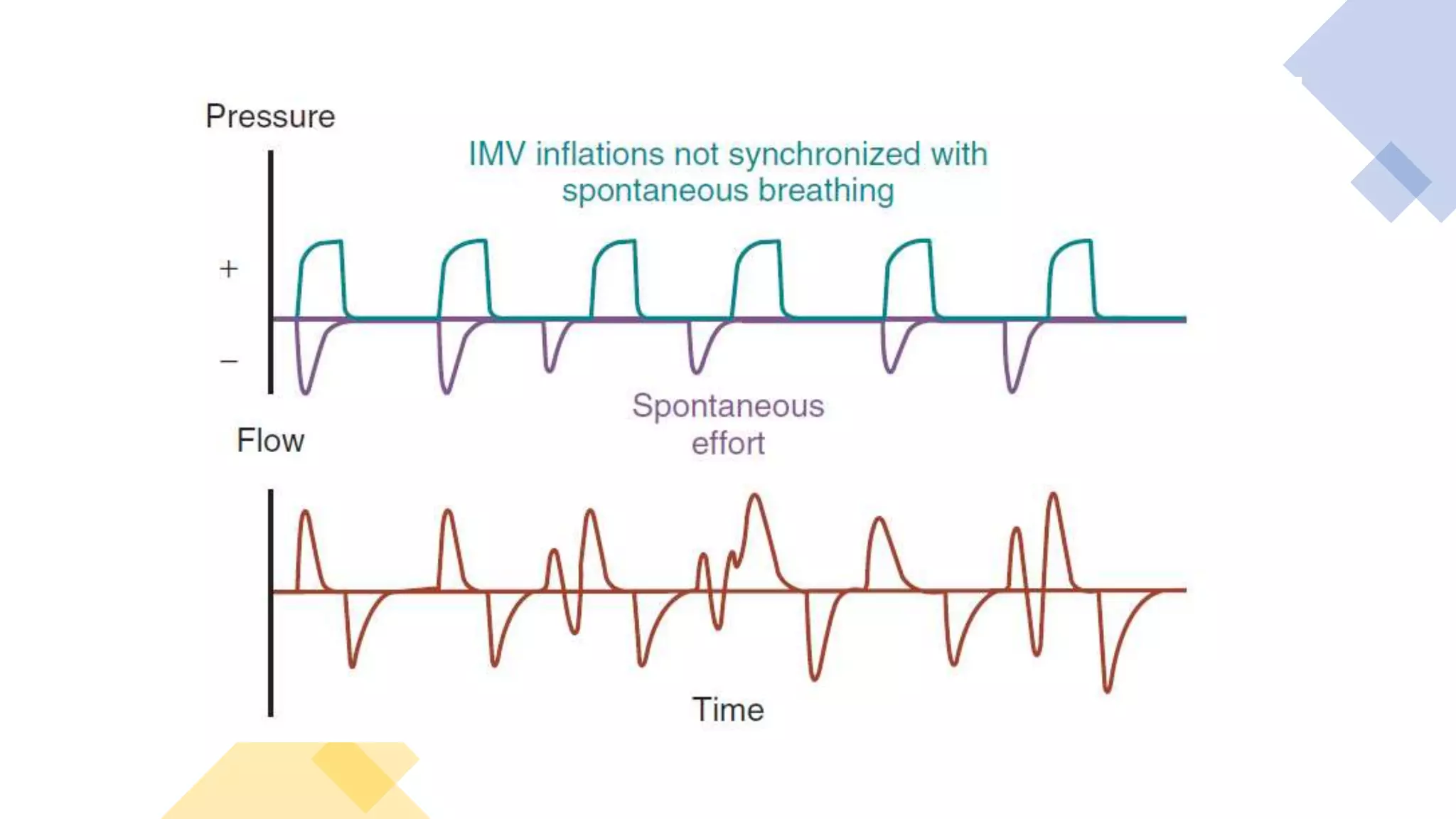
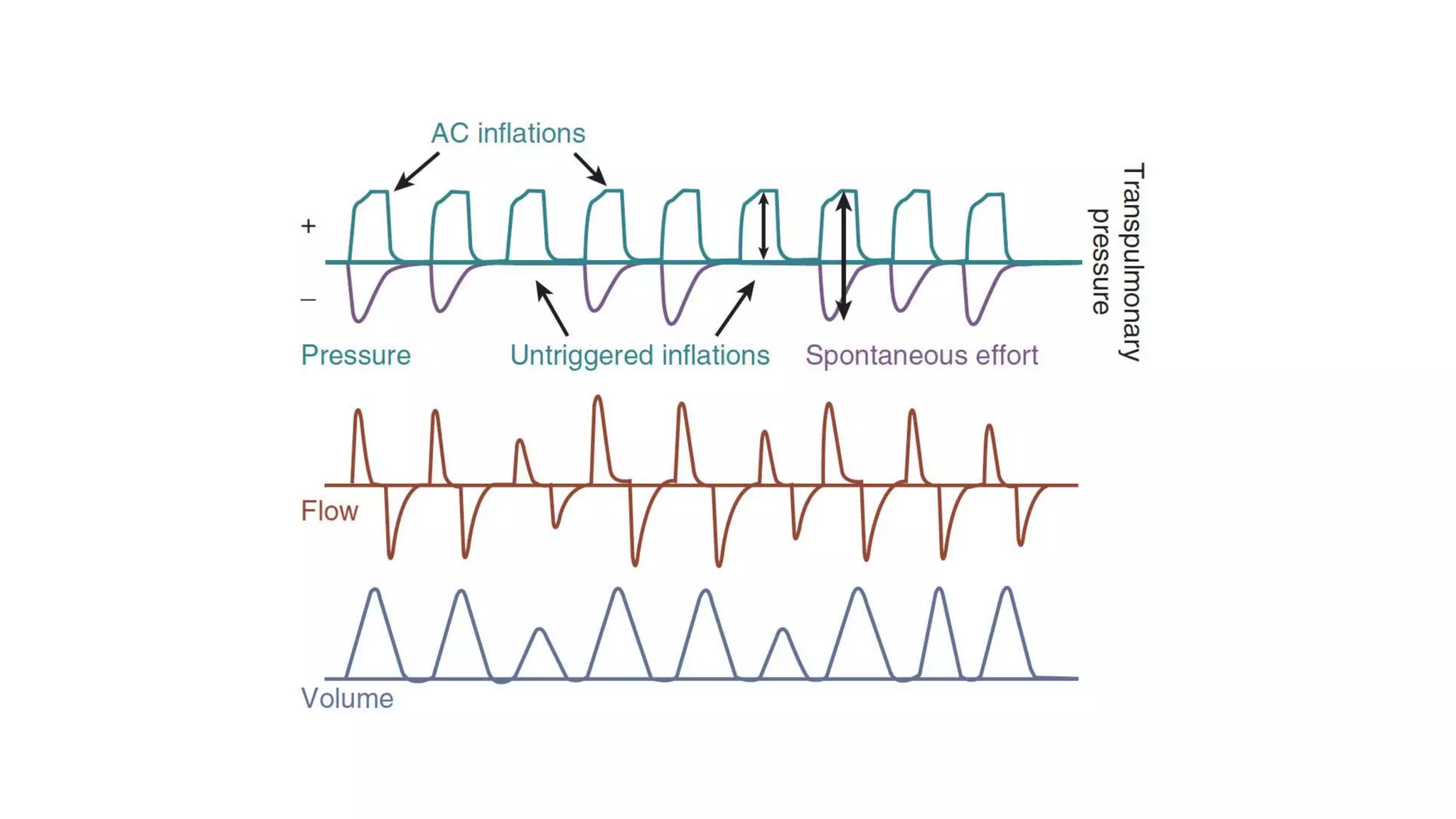
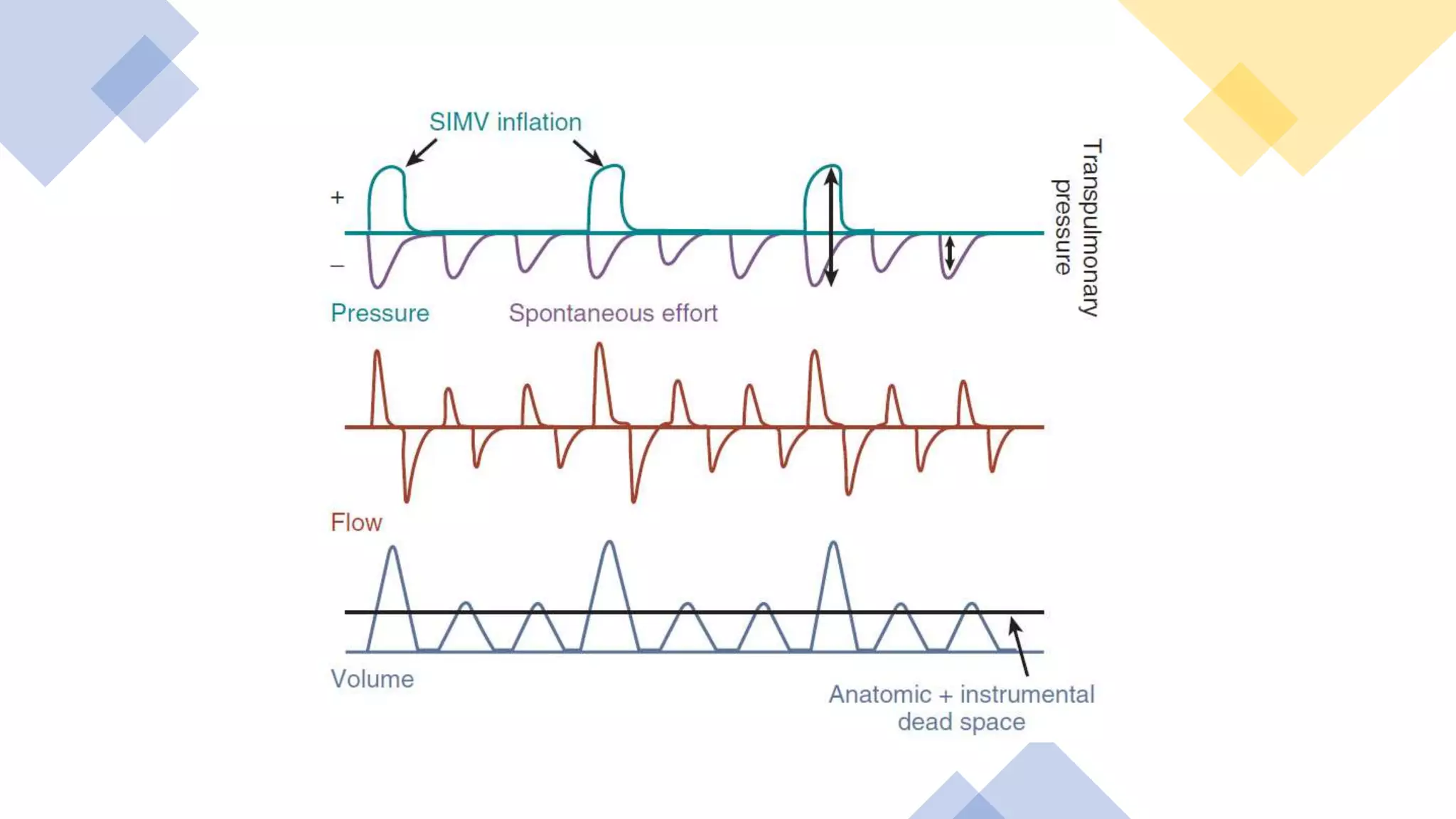
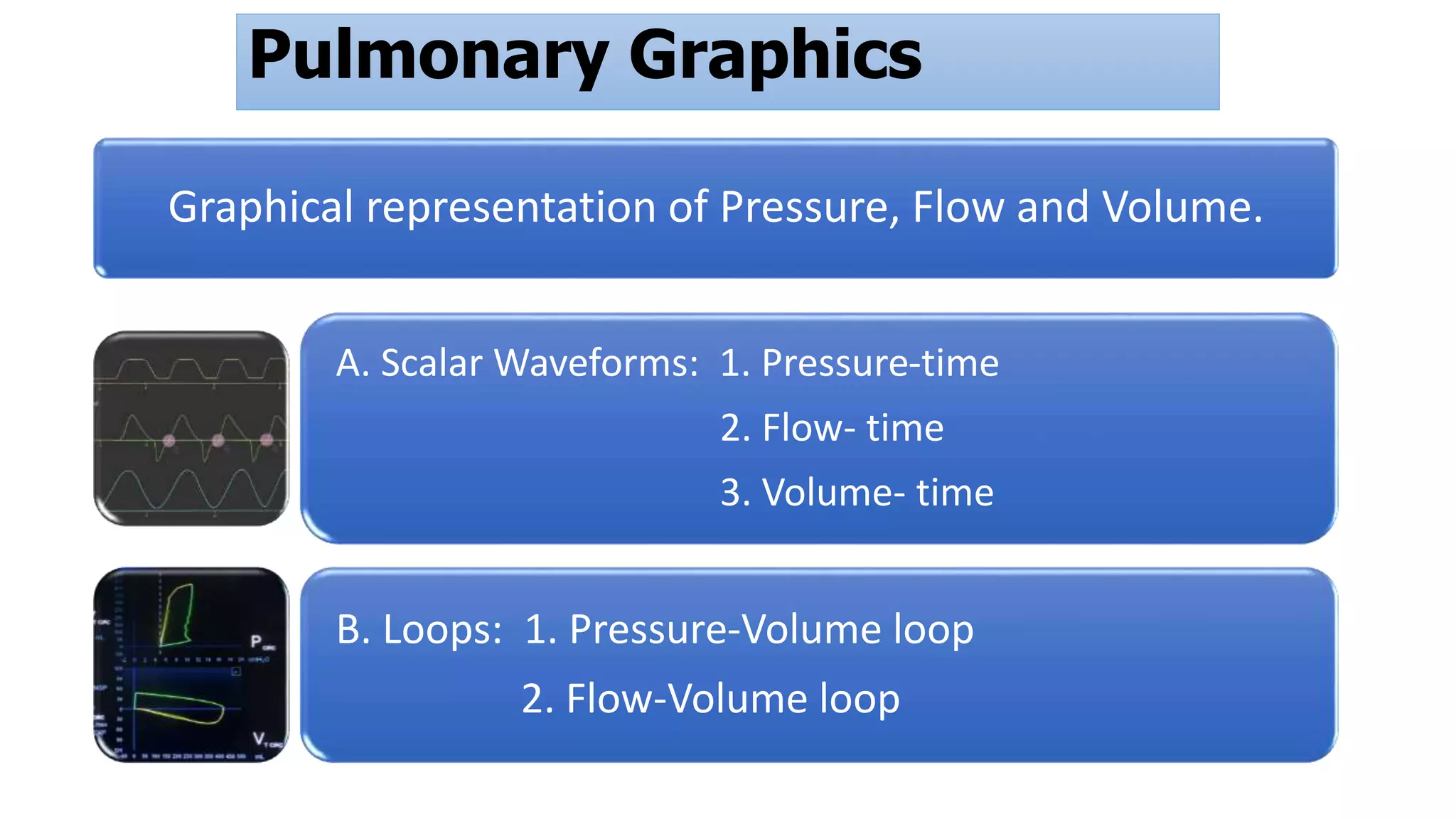
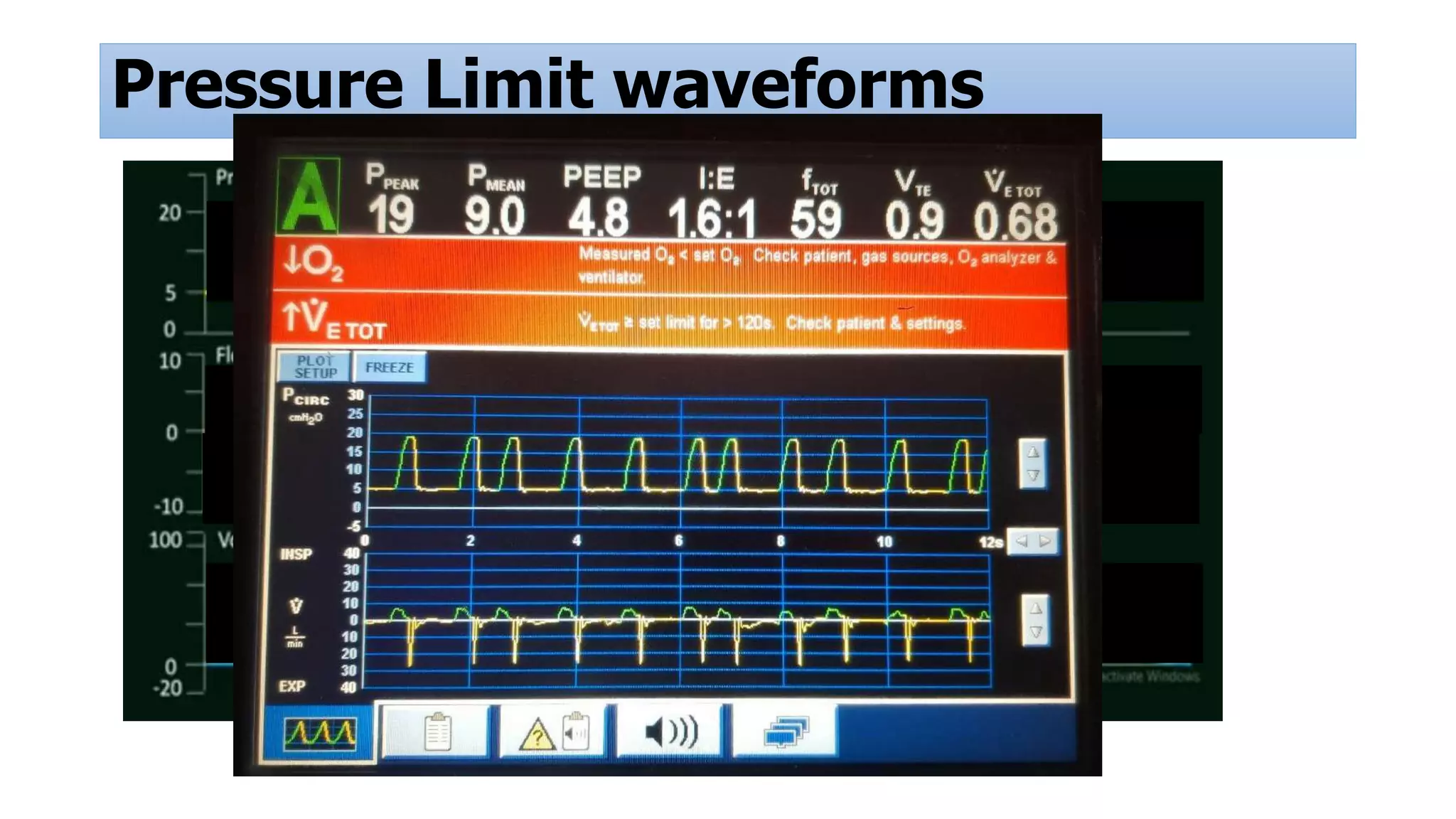
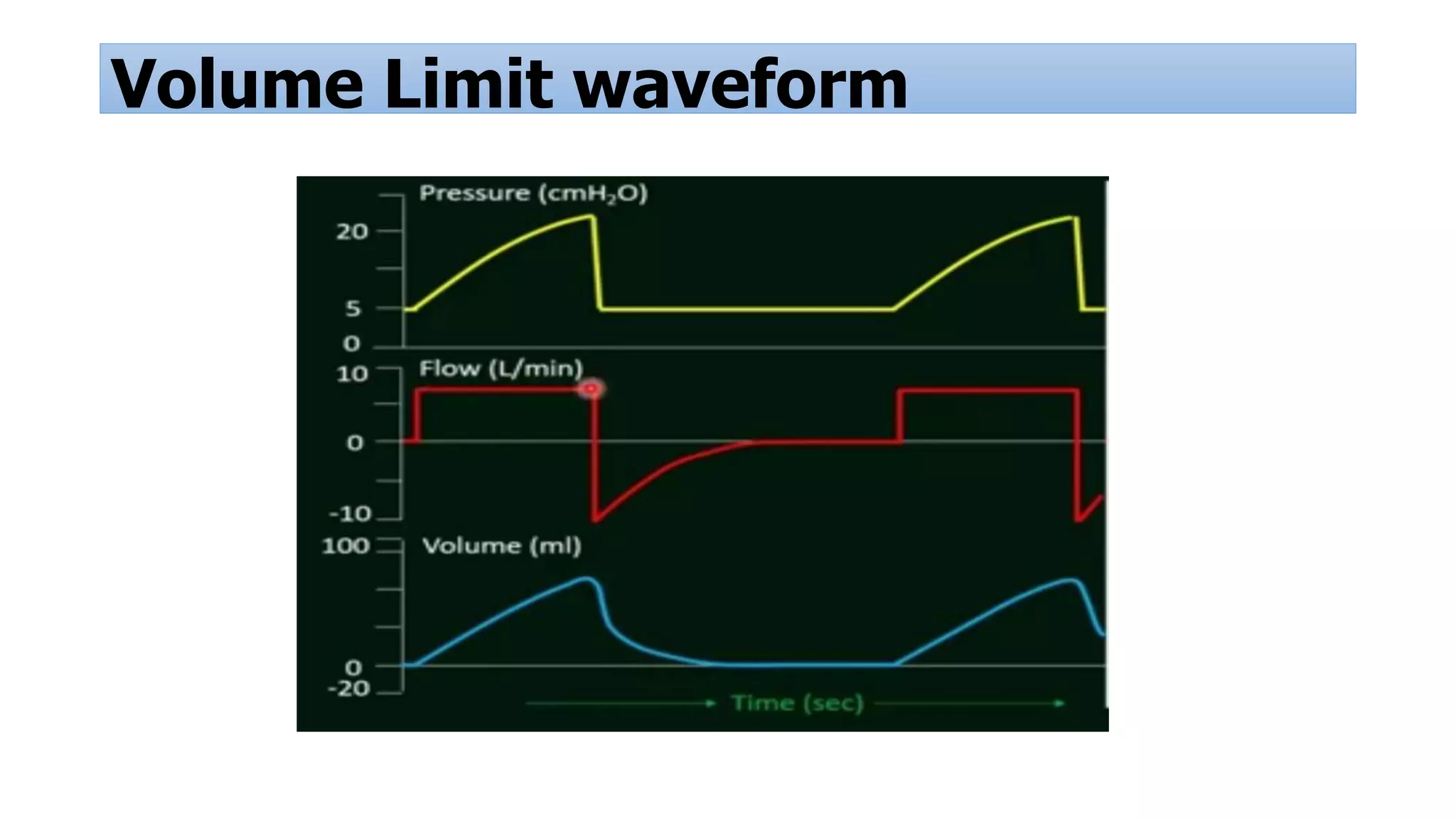
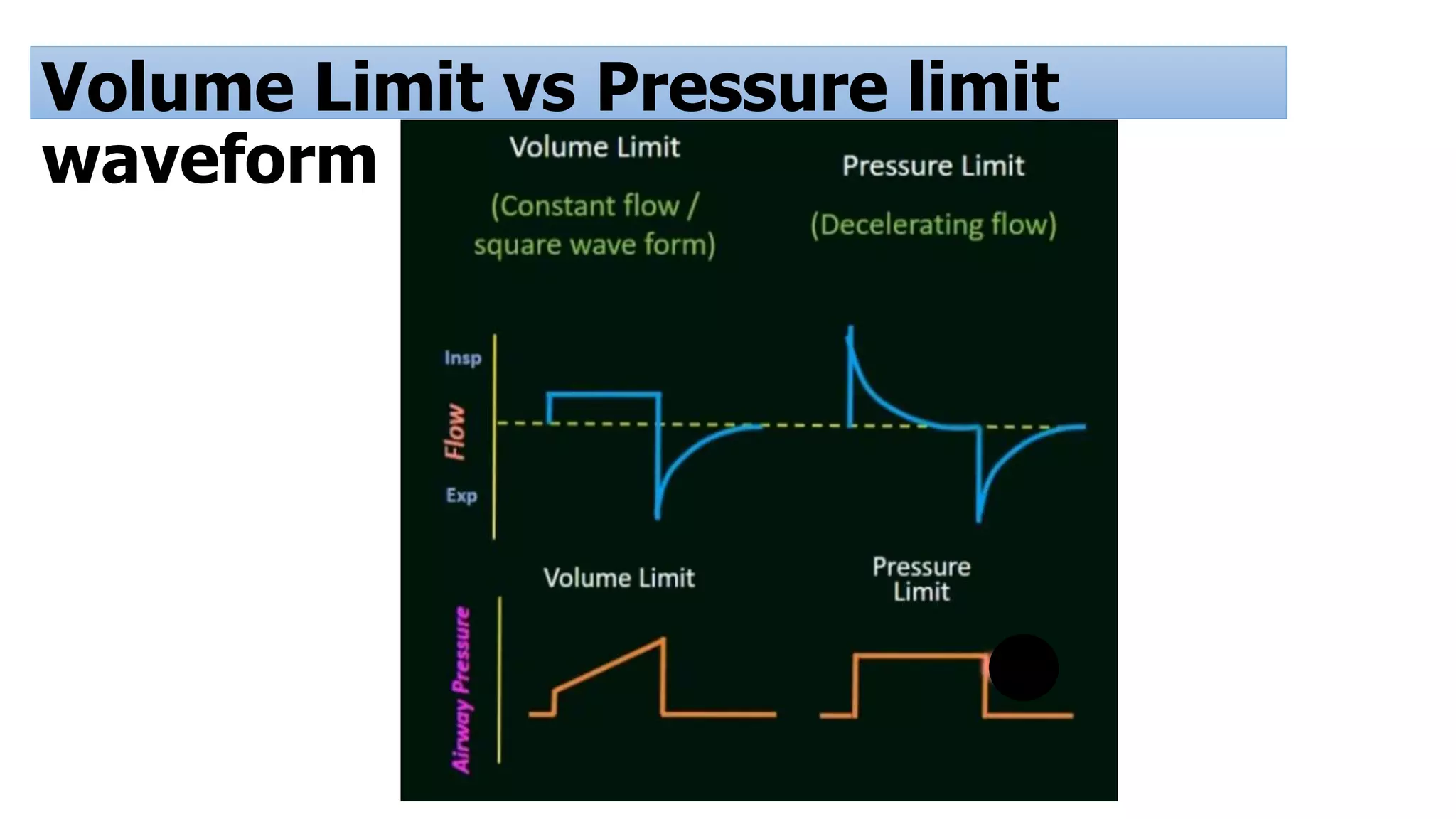
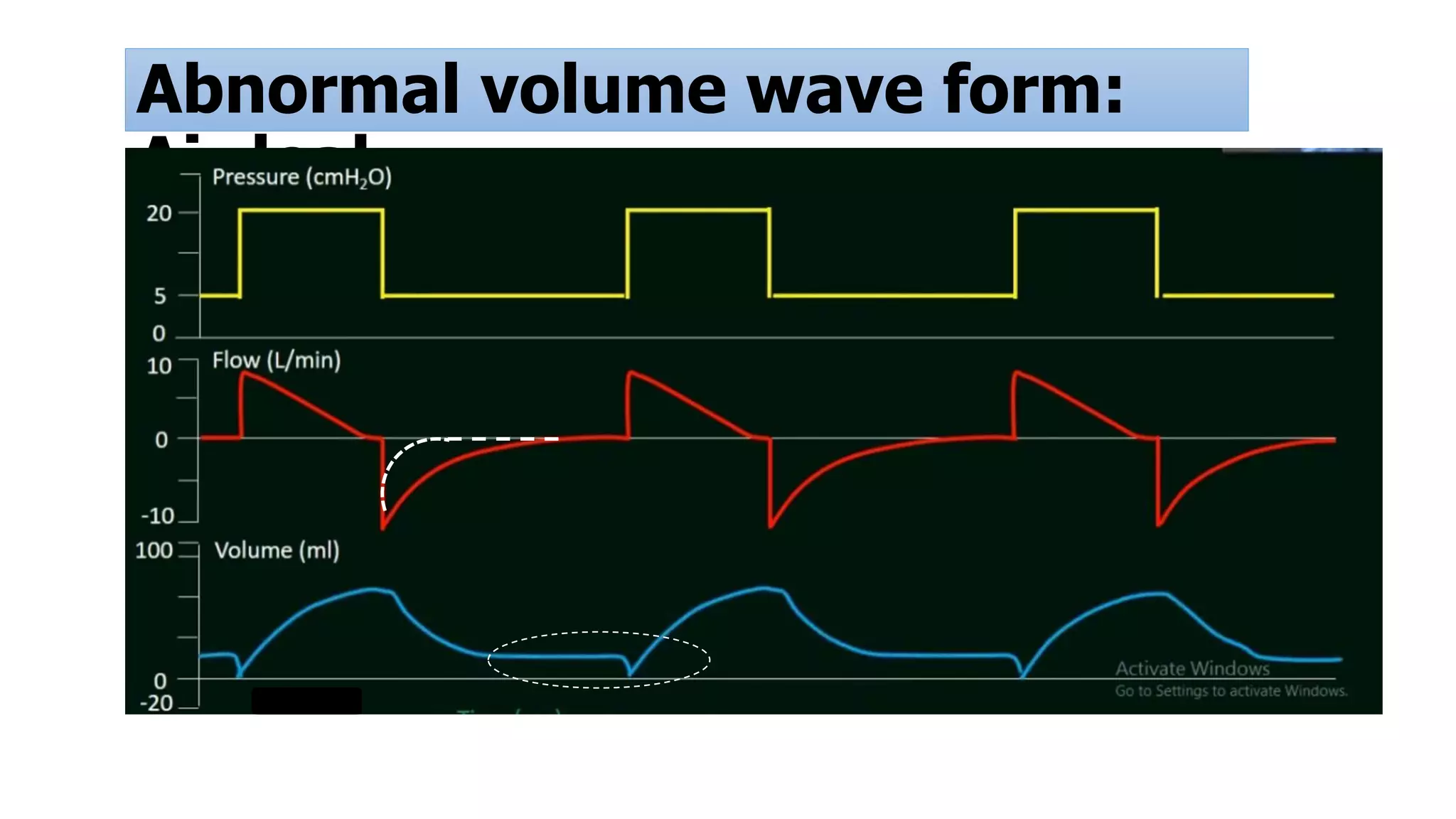
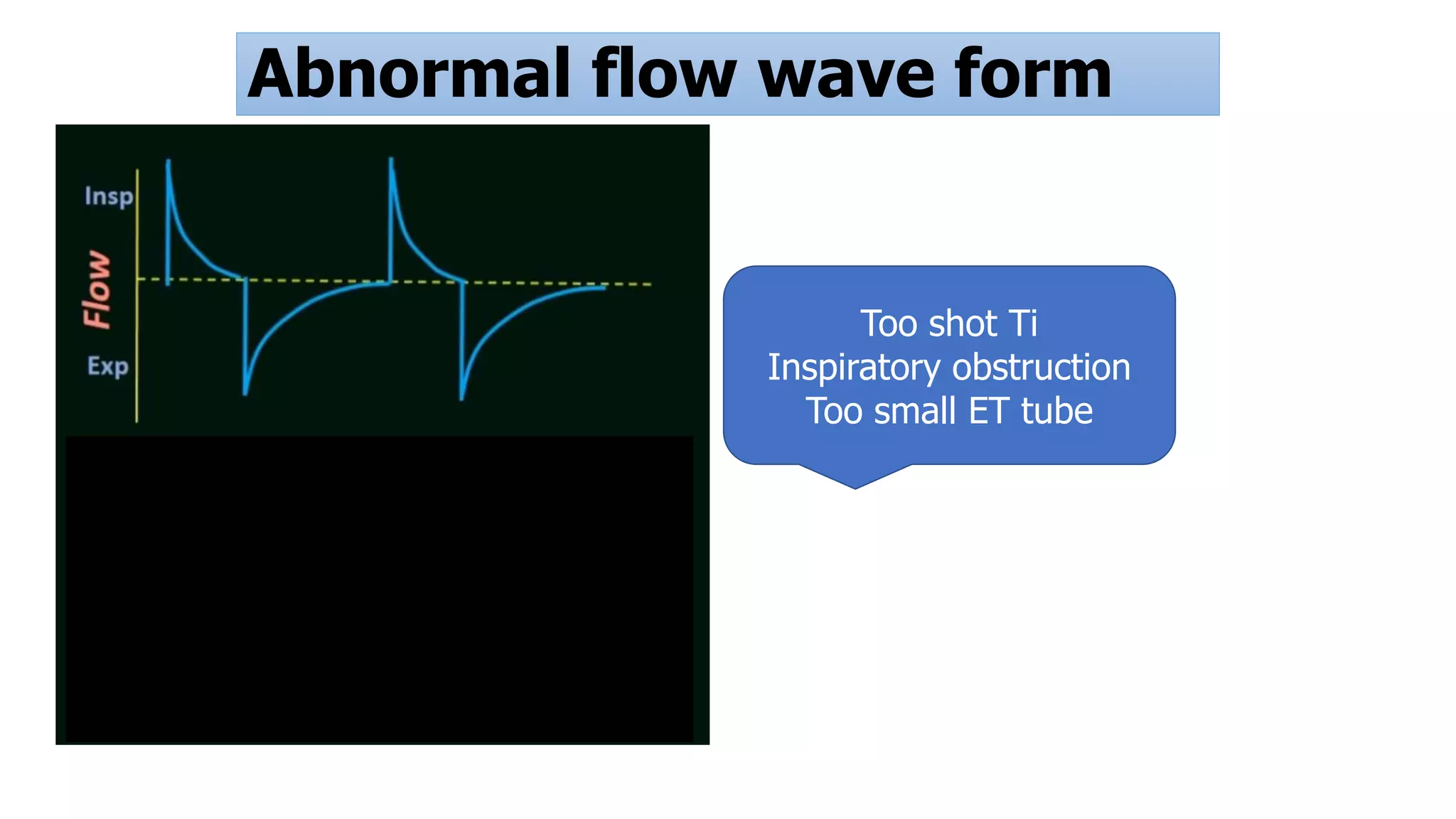
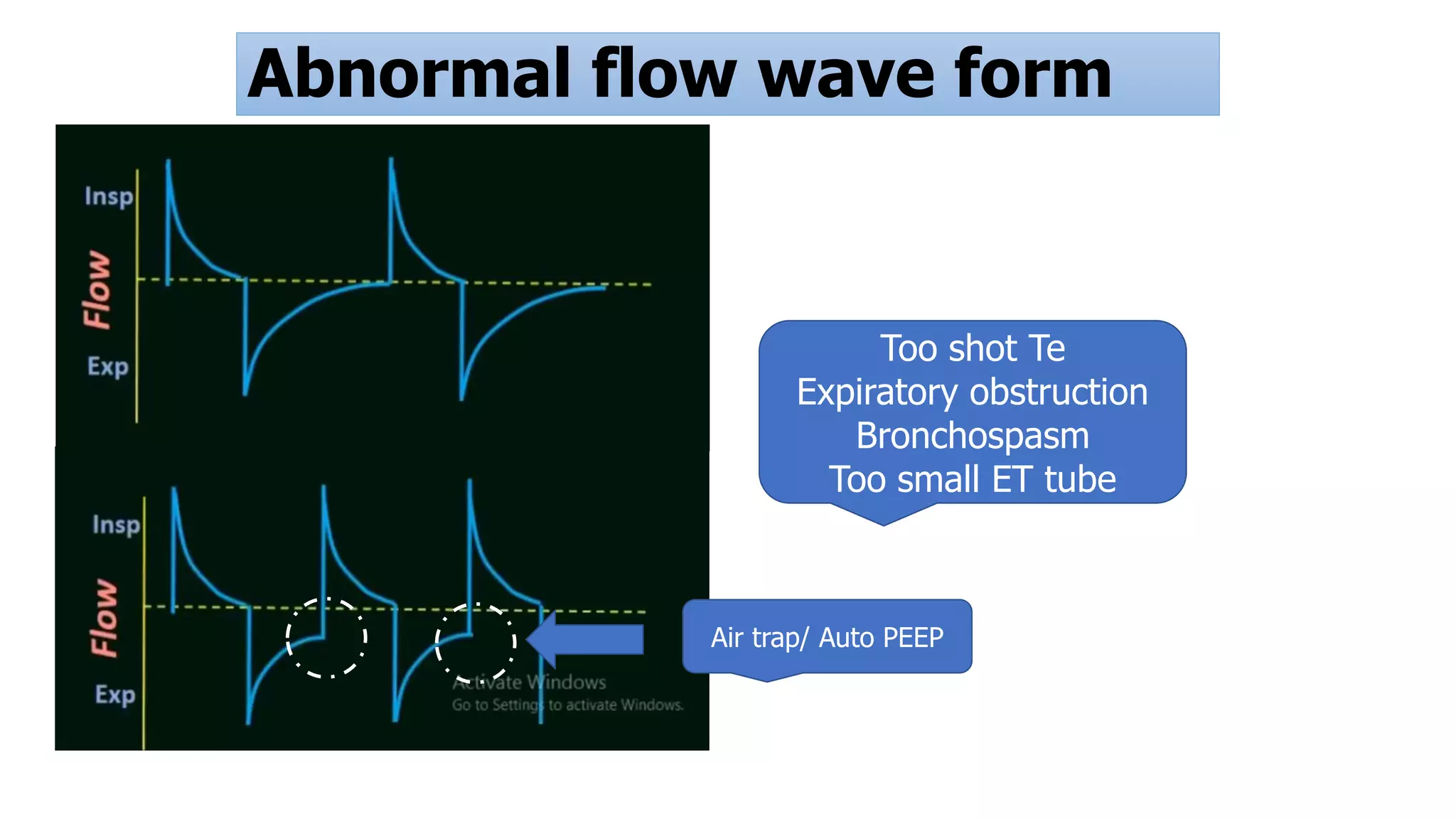
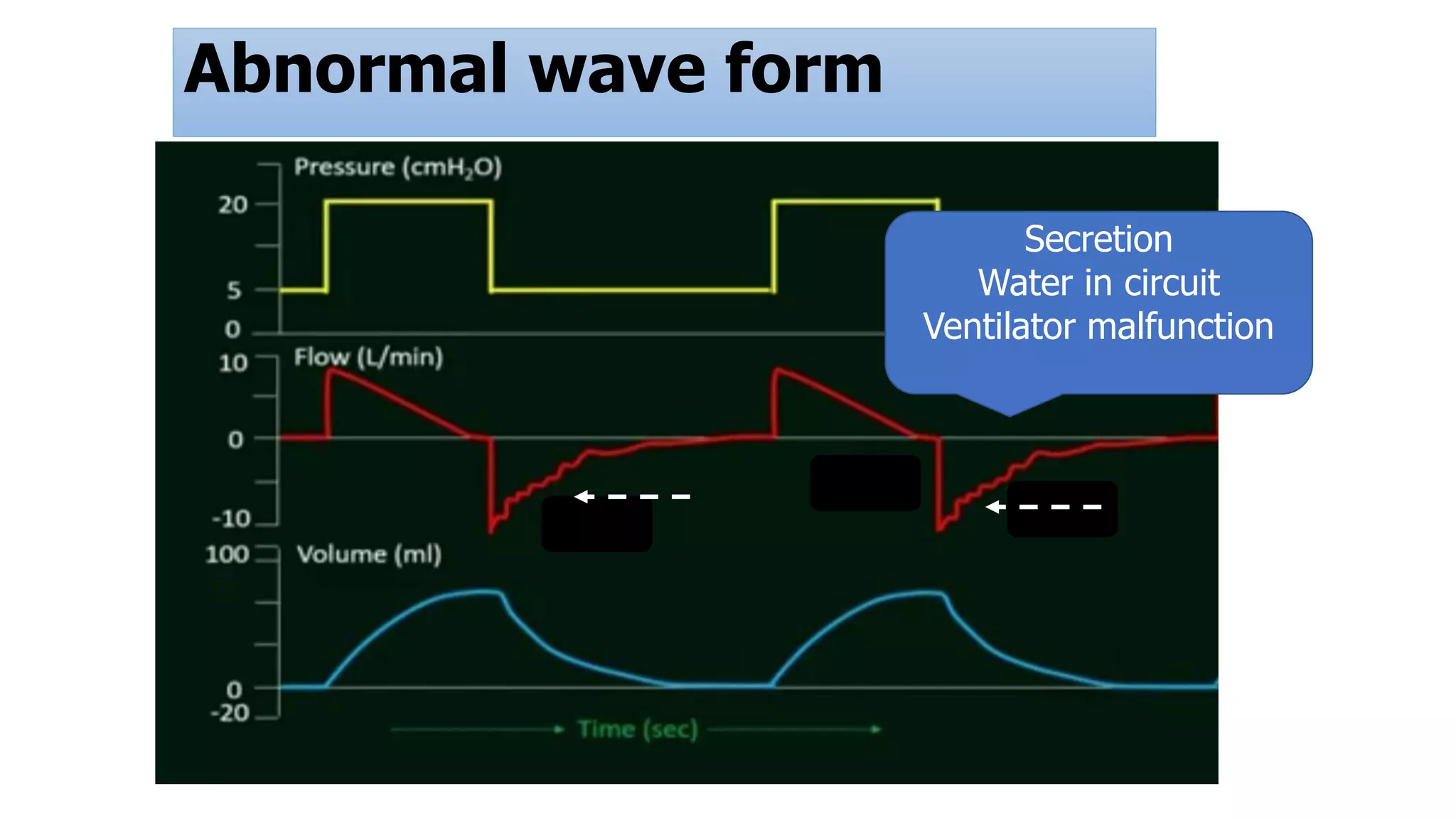
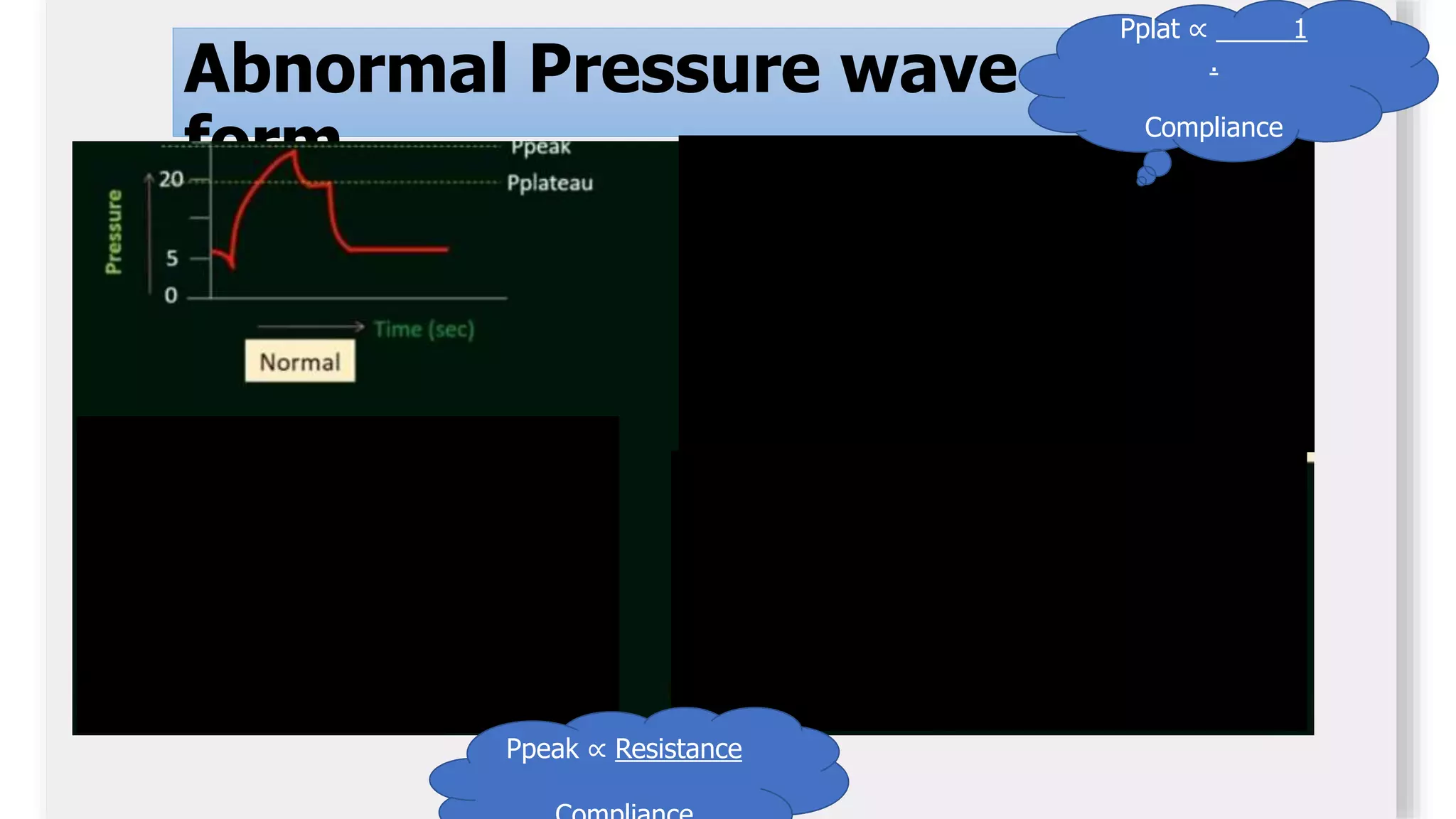
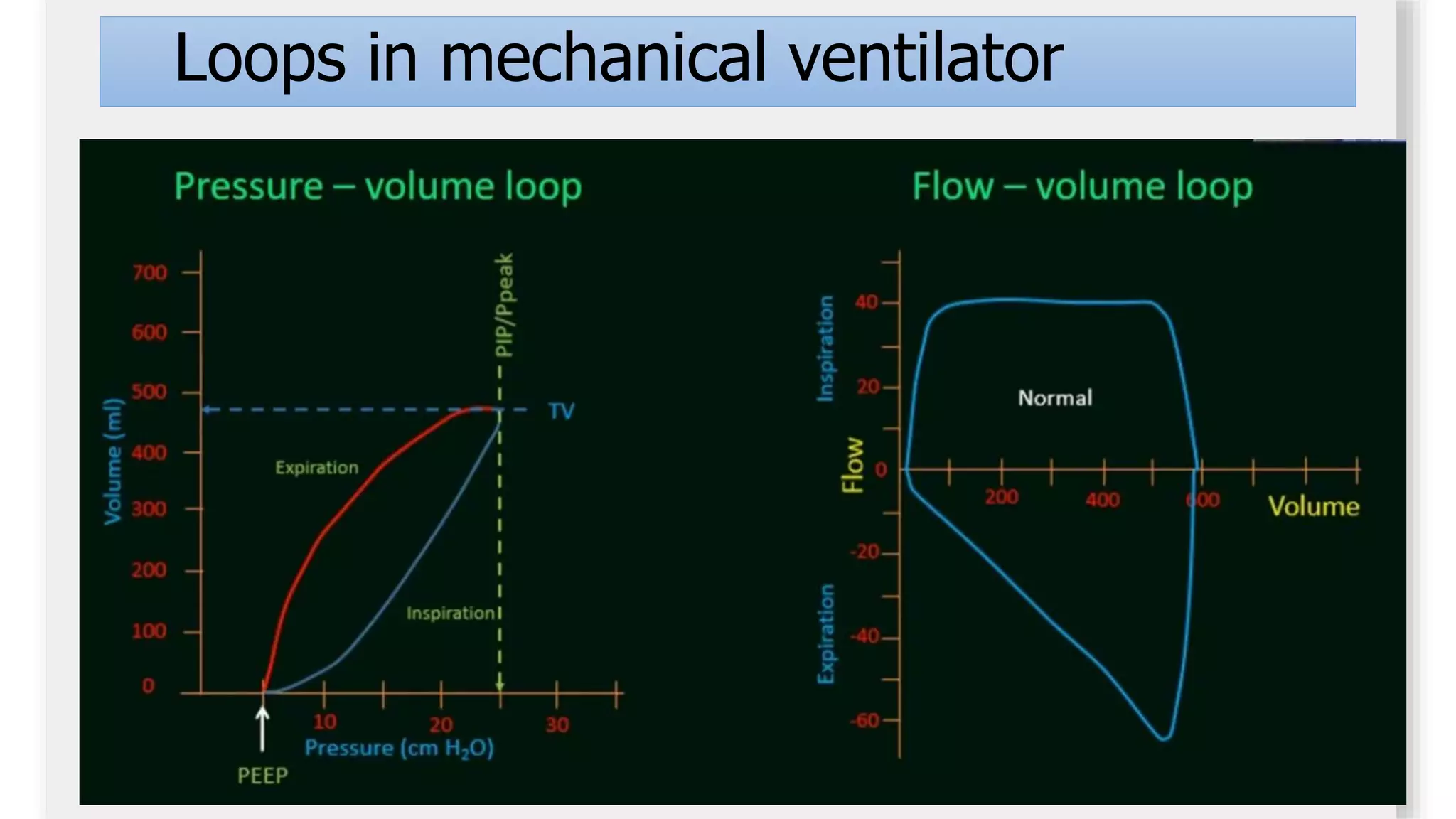
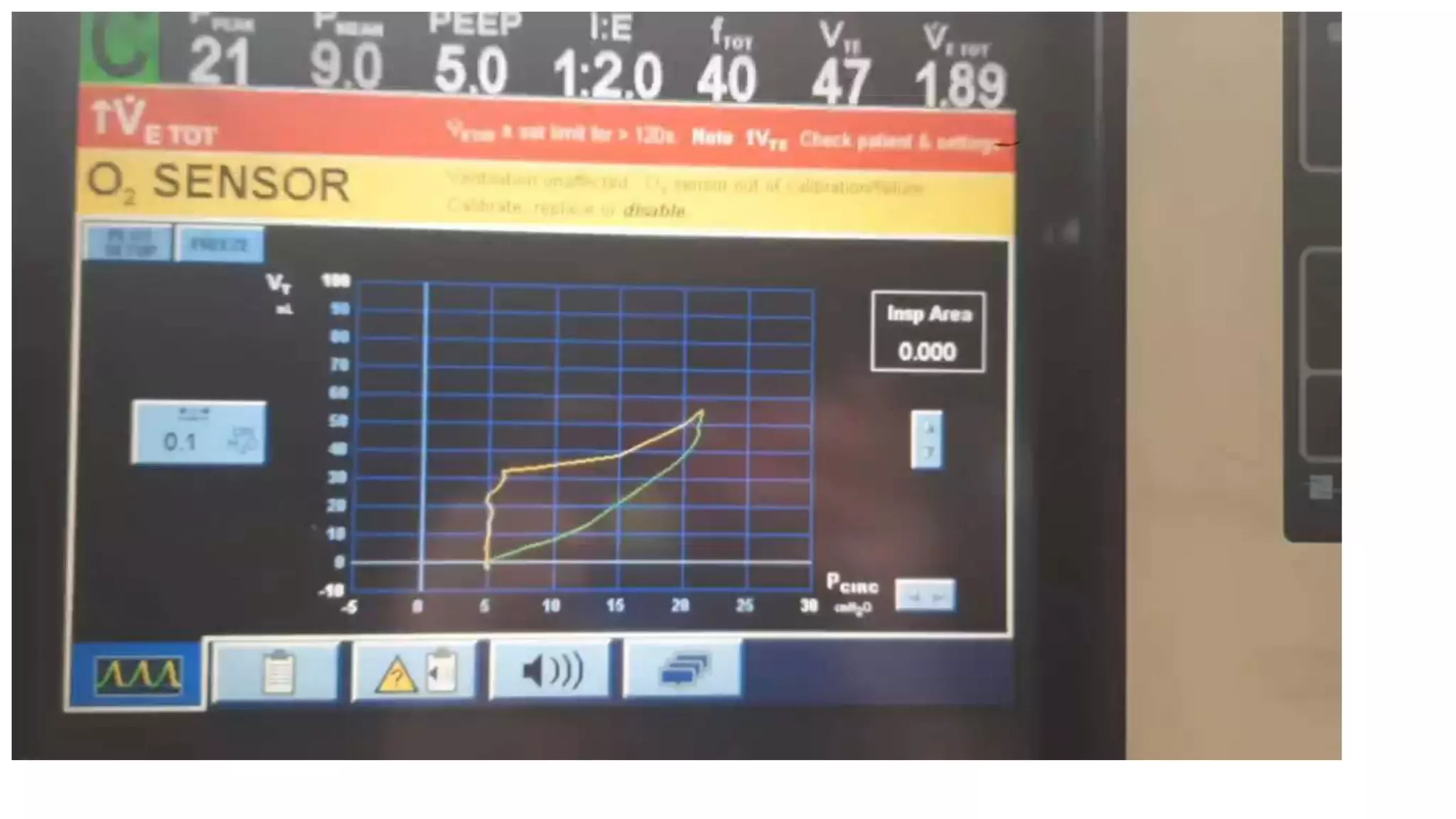
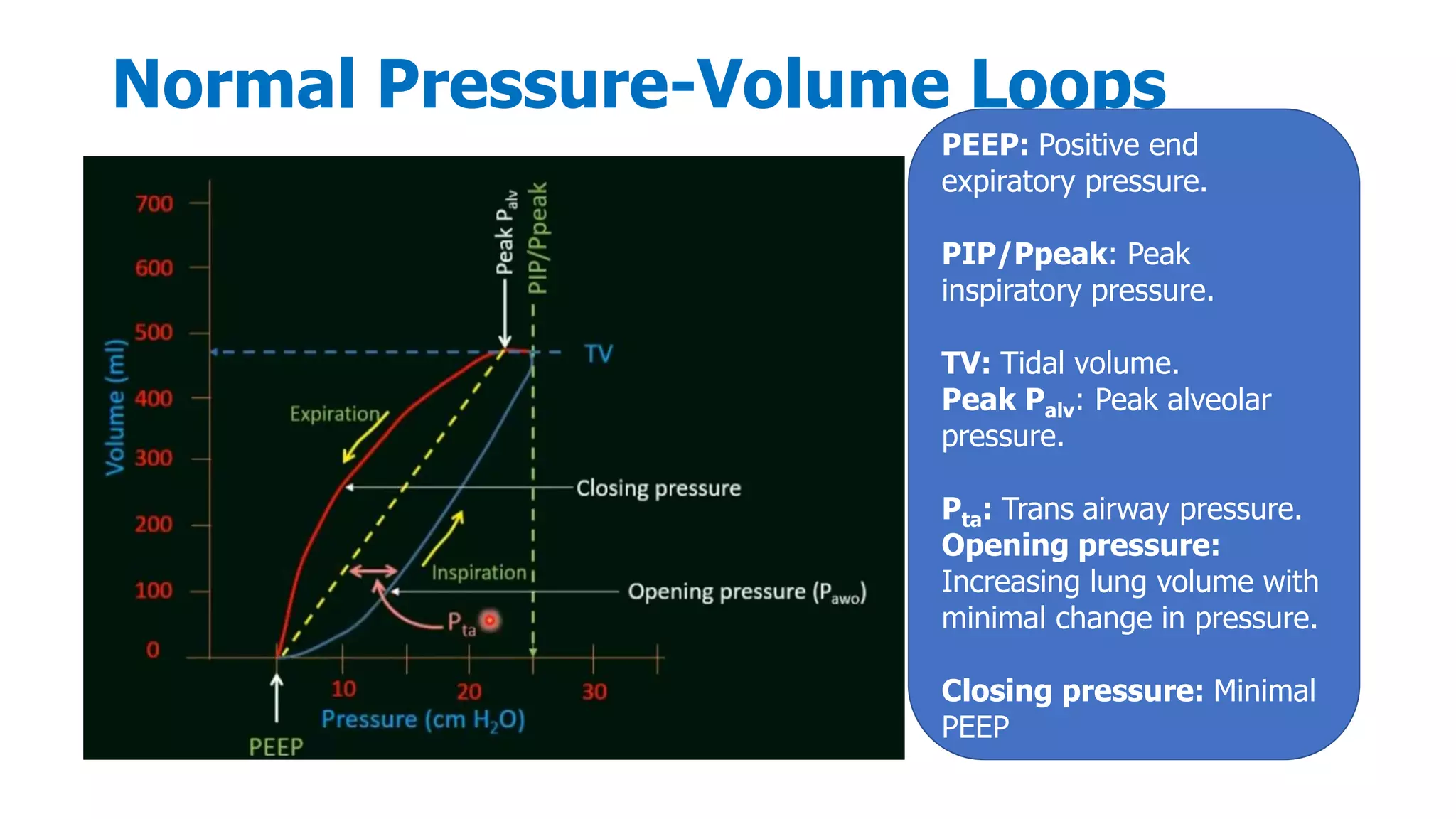
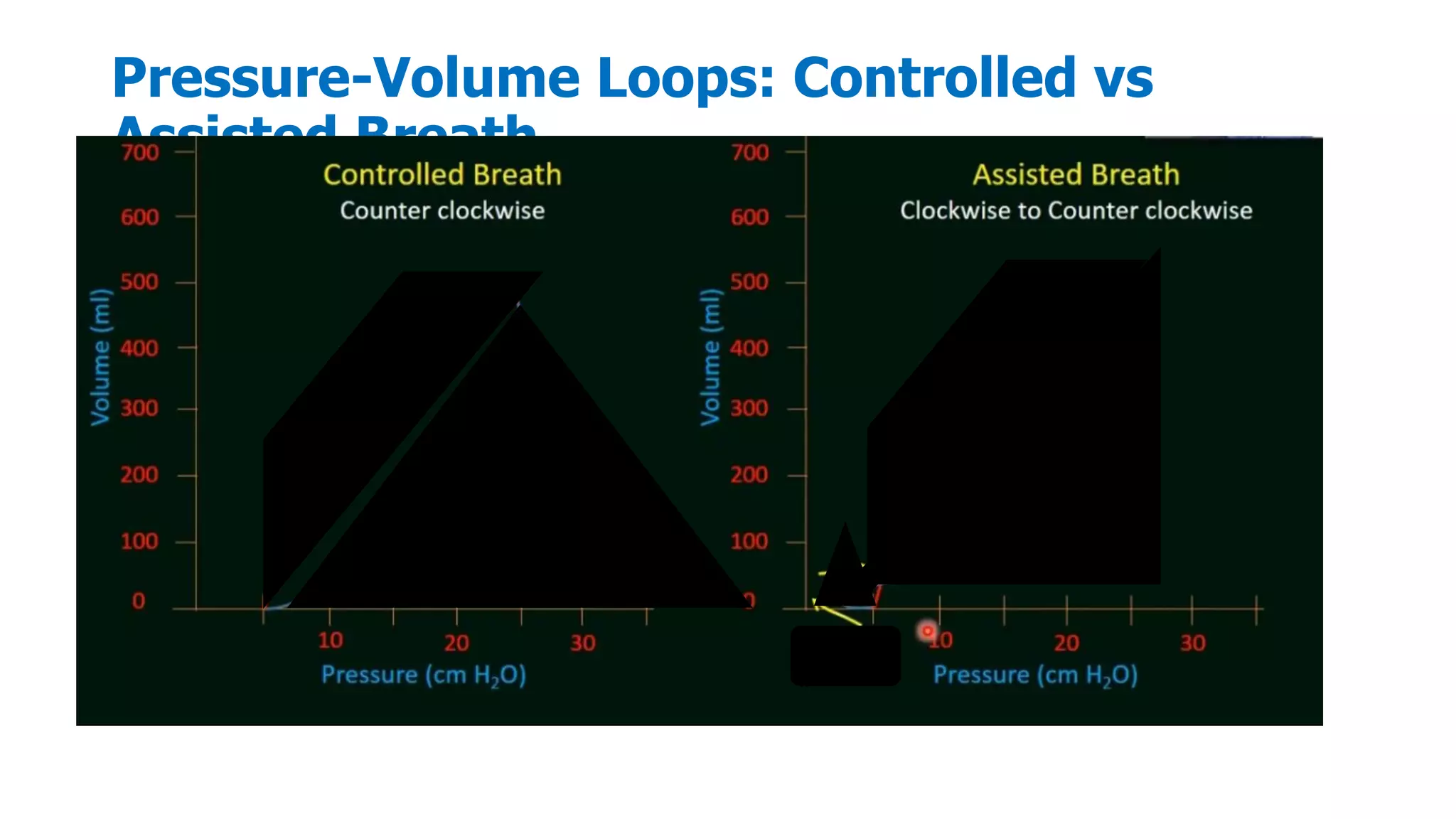
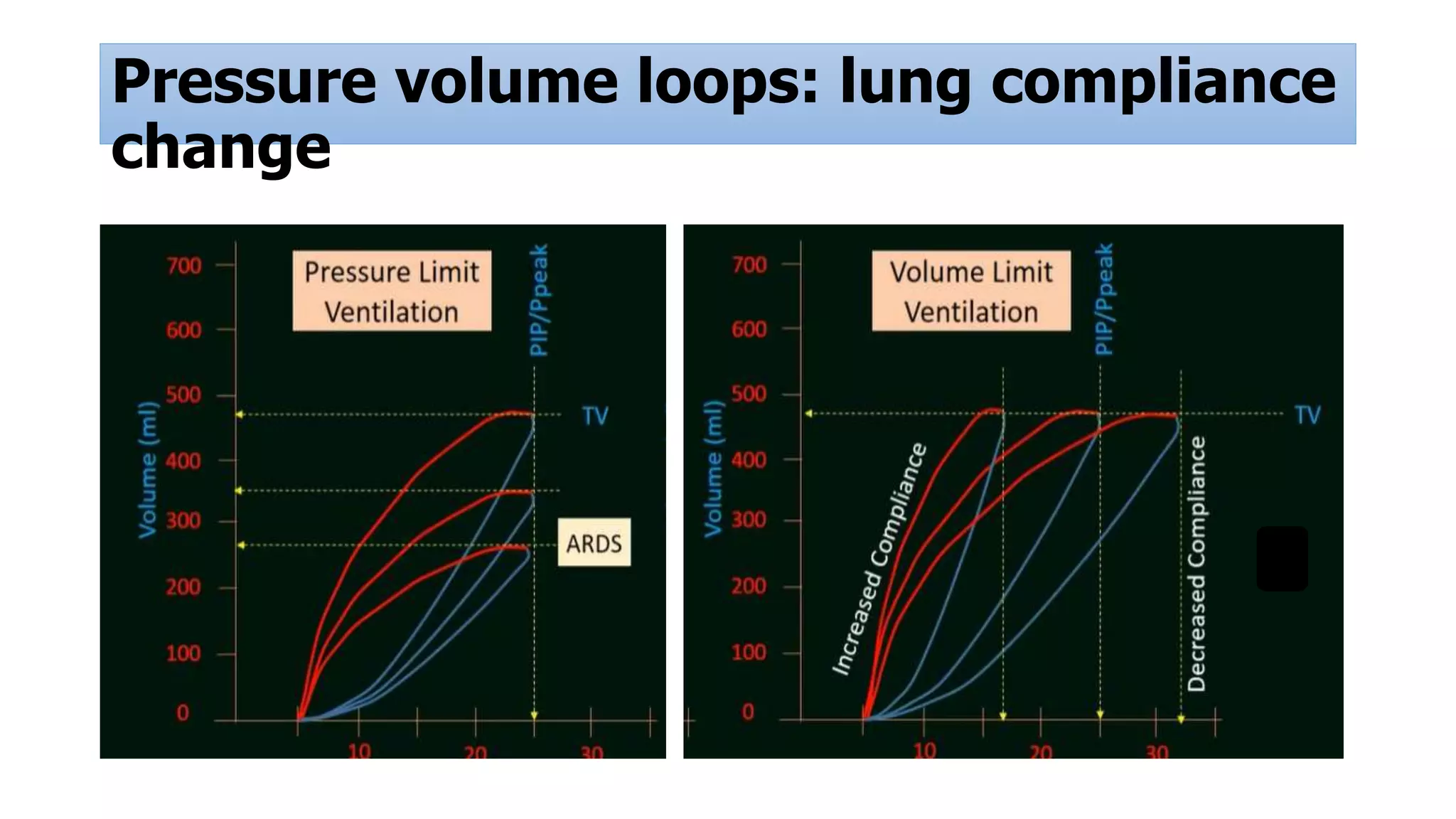
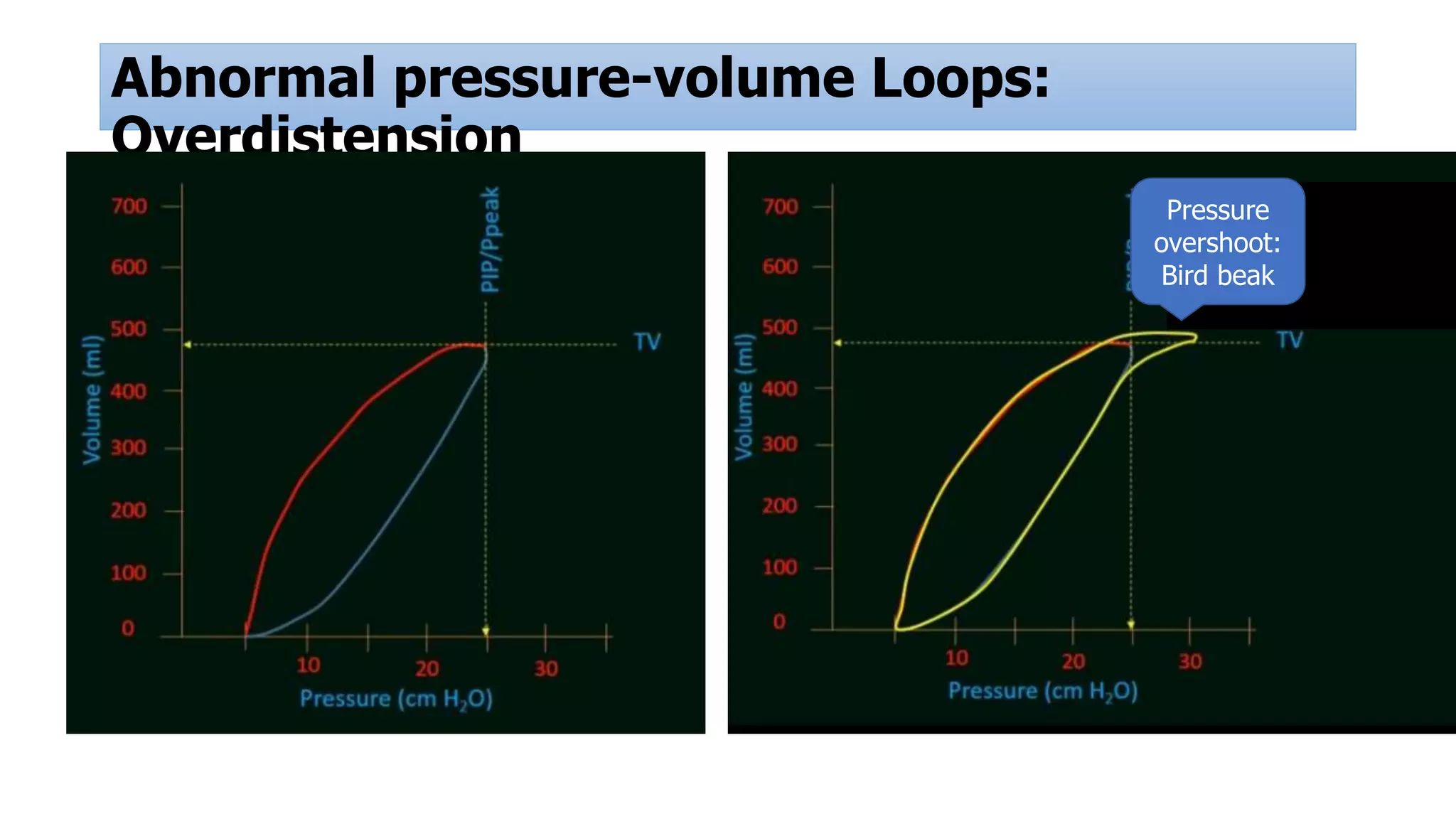
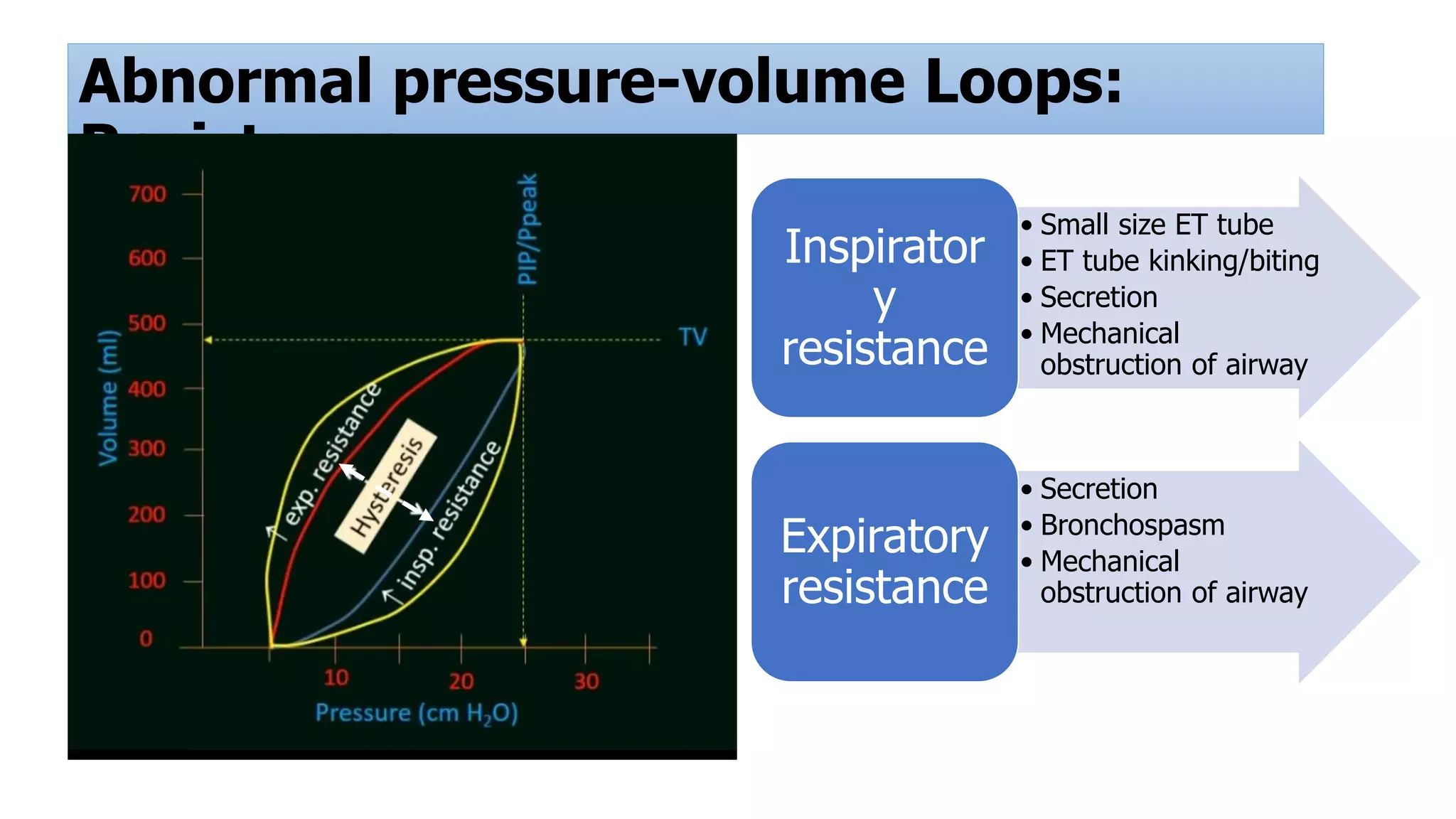
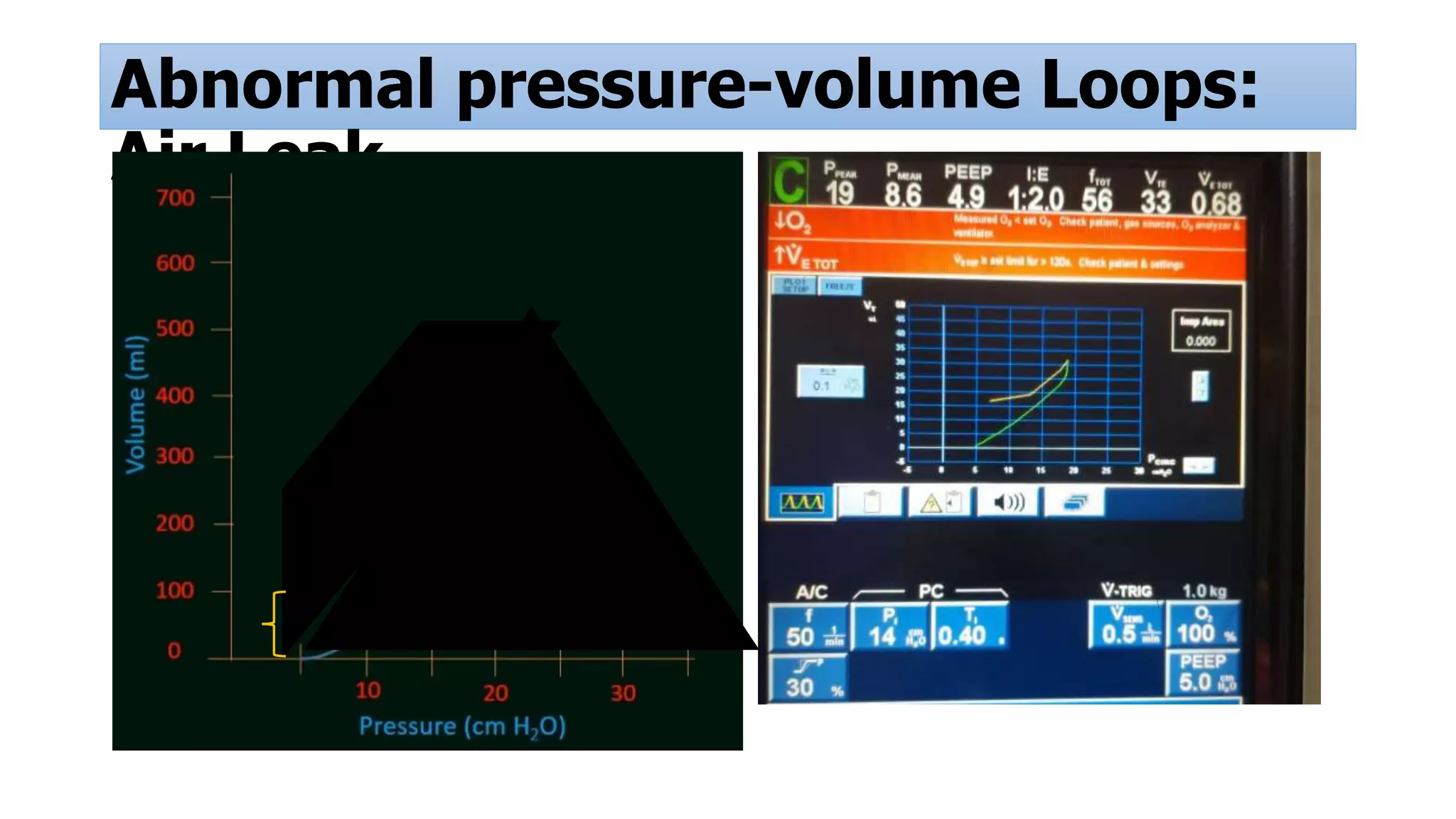
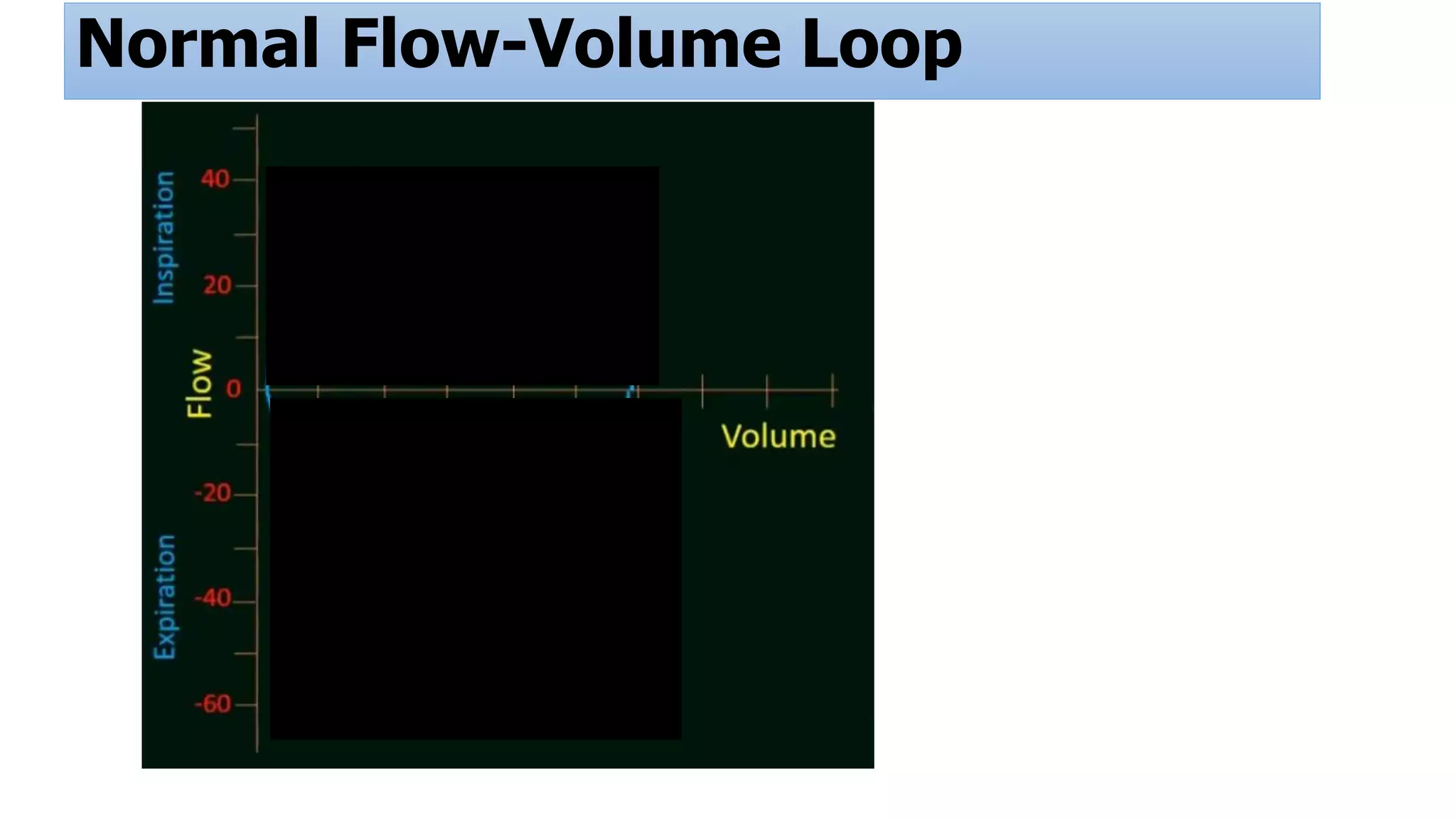
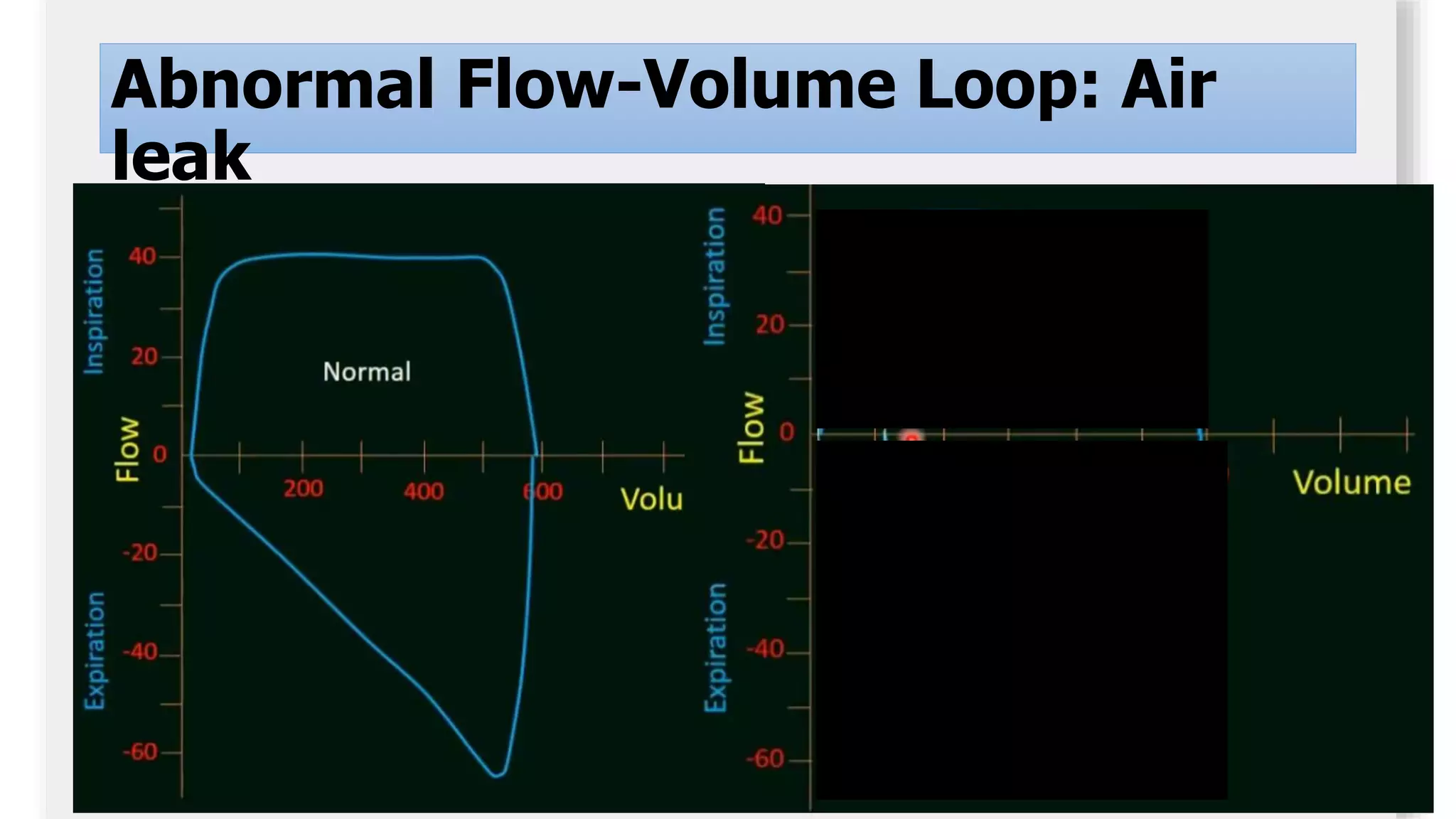
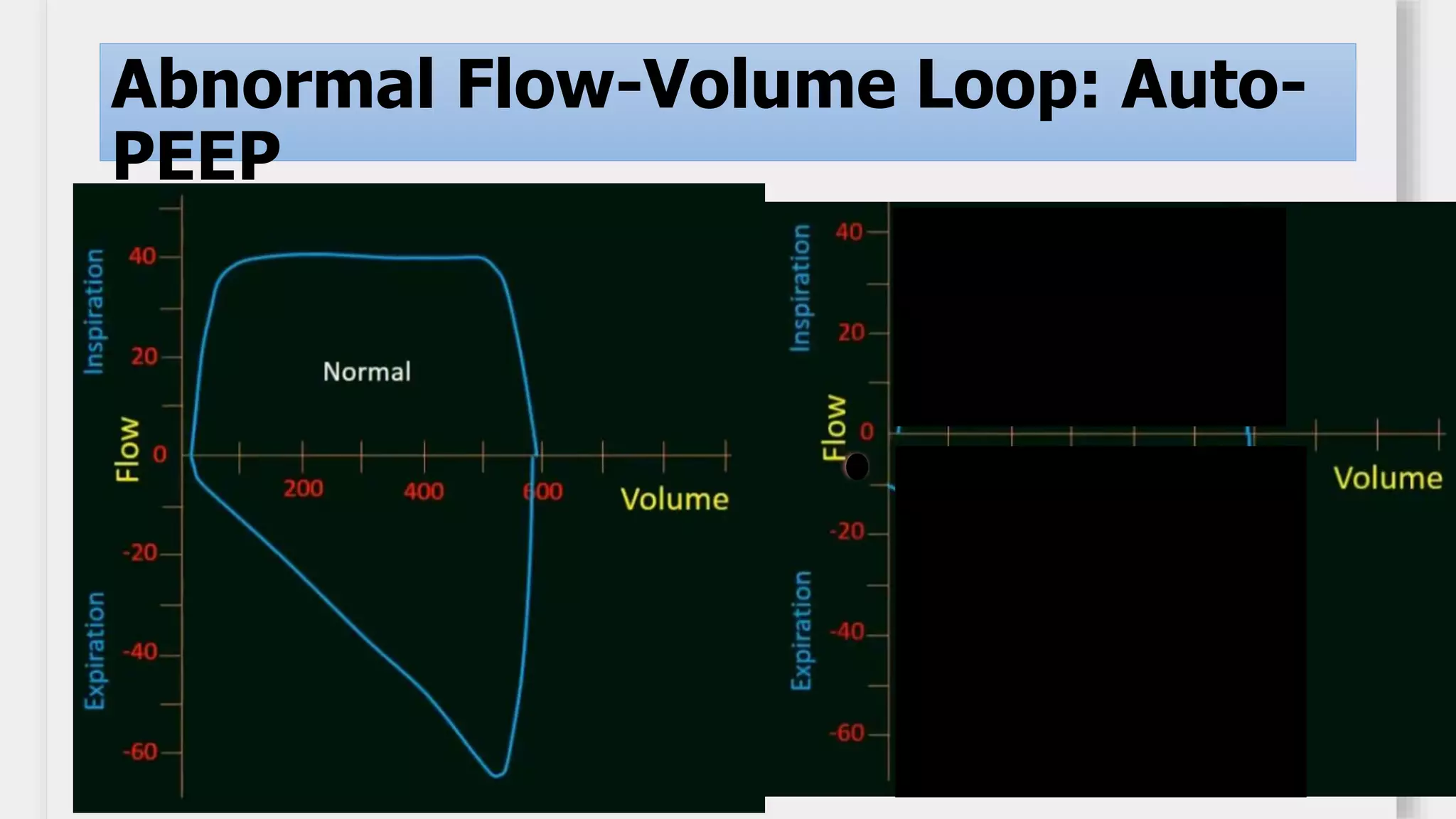
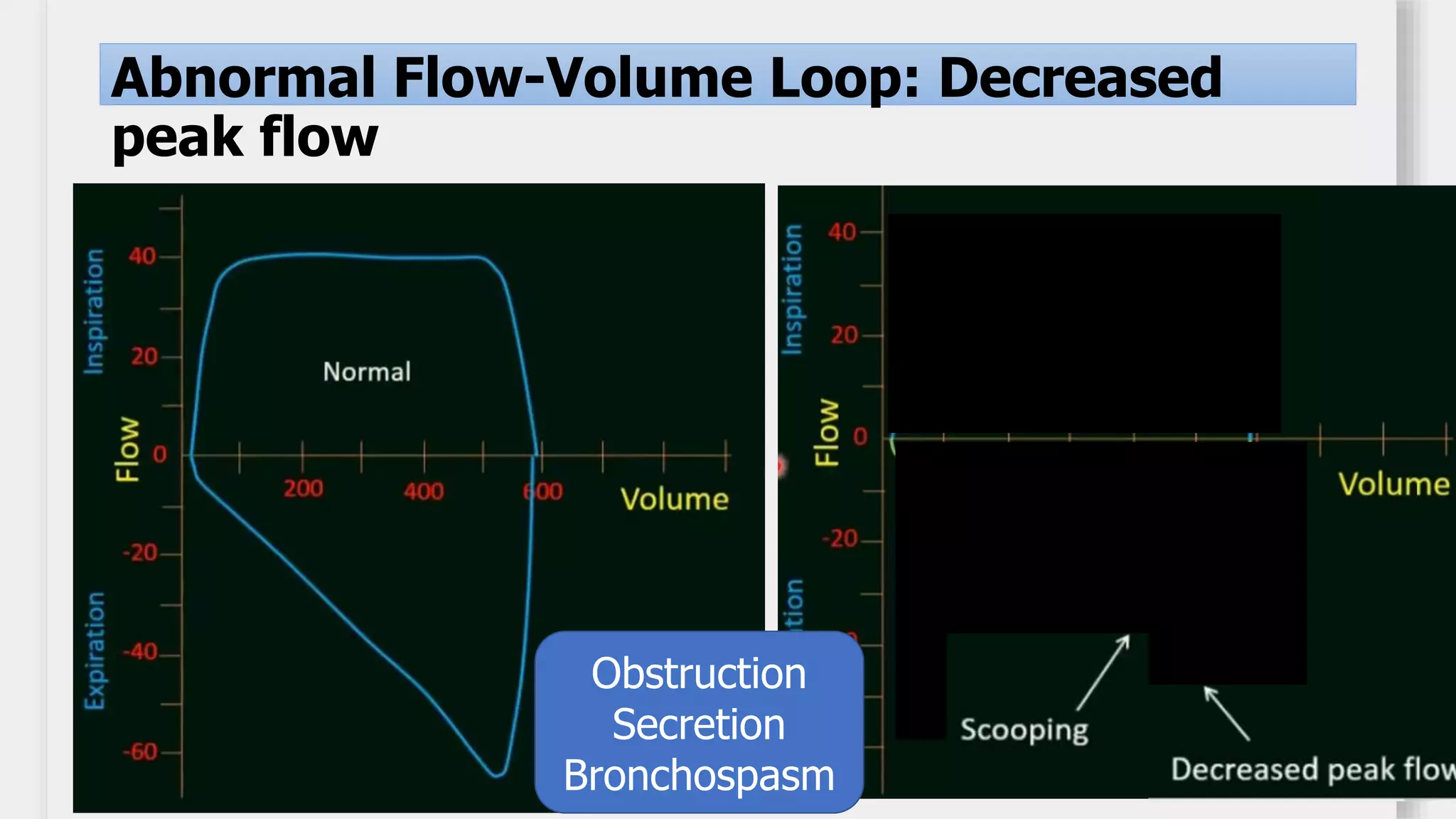
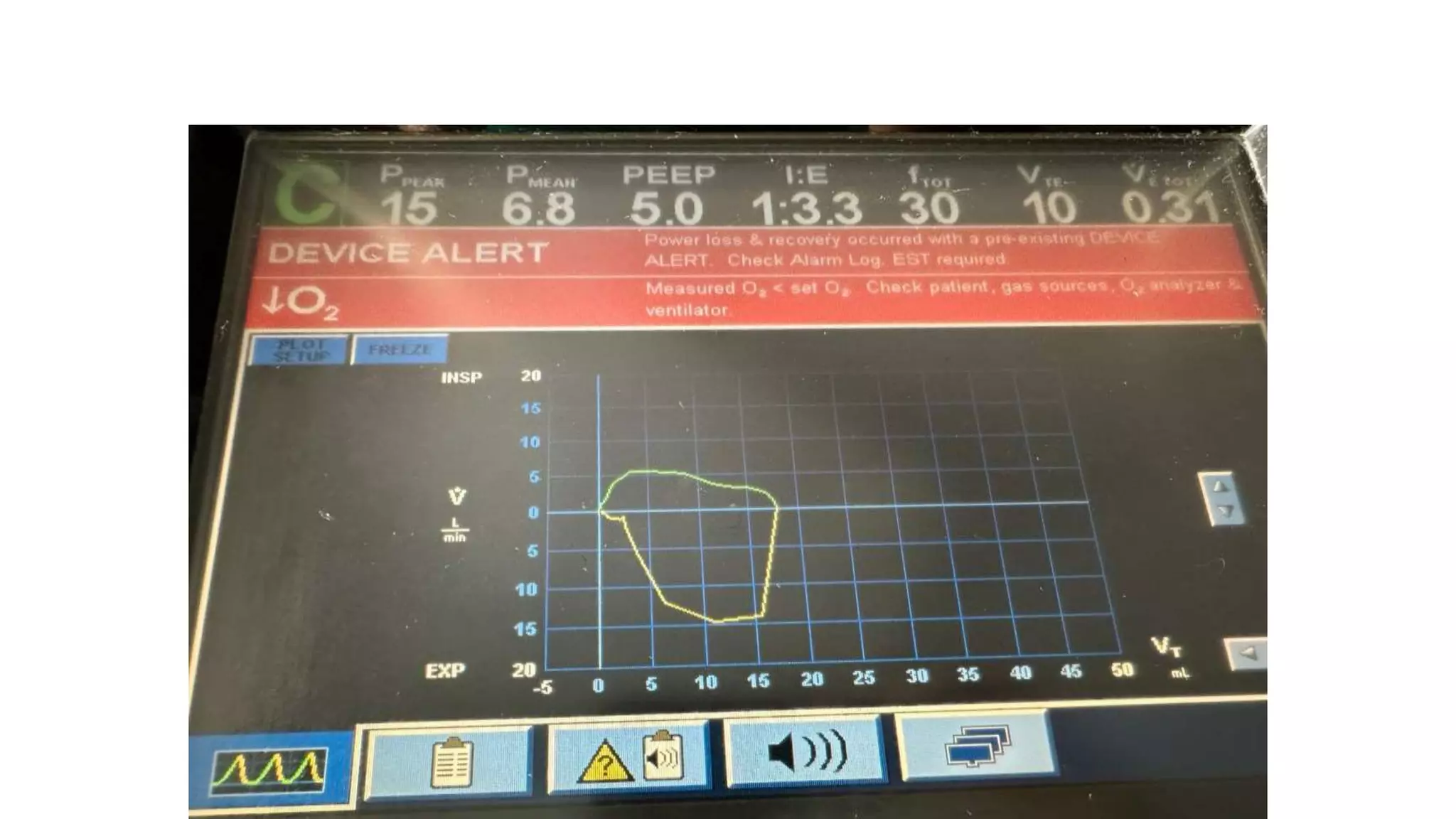
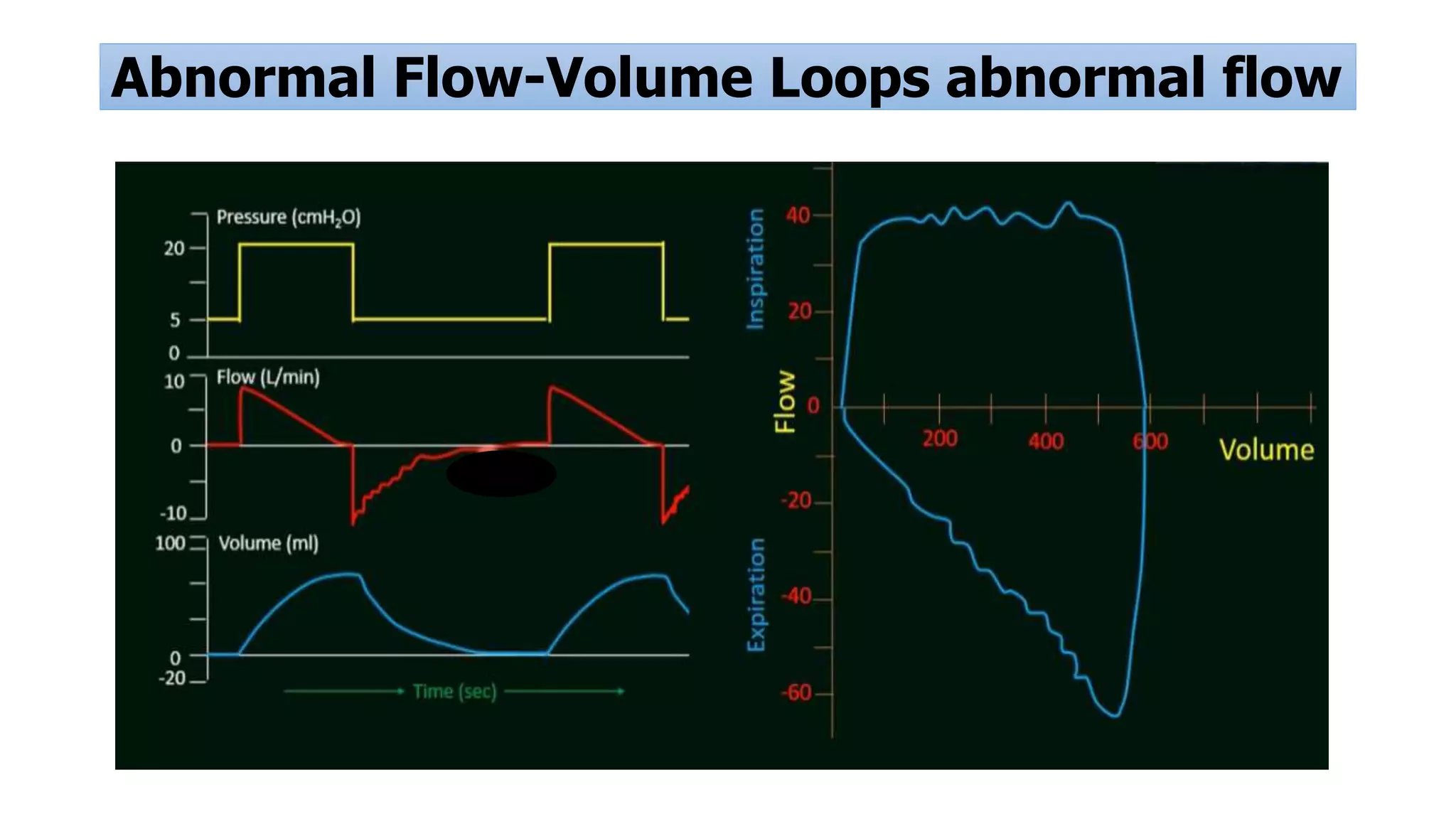
Graphical representation of ventilatory parameters, abnormal waveforms indicating issues like air leak or obstruction.
Overview of specific ventilators used in neonatal care, including Dräger and Babylog models.























































































