Downloaded 16 times
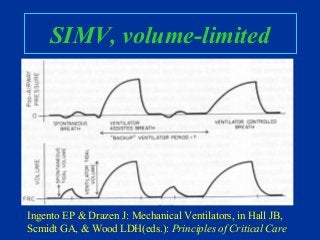
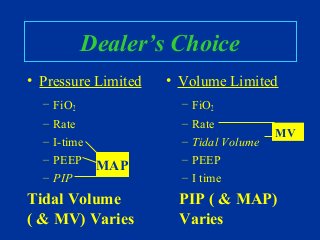
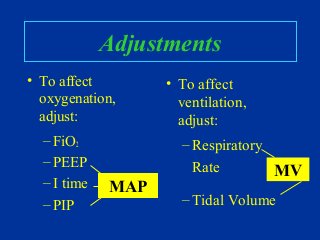

This document provides an overview of mechanical ventilation including: - Indications for mechanical ventilation including respiratory and cardiac failure. - Basic anatomy and physiology of ventilation including the roles of airways, alveoli, and pressures. - Common modes of ventilation like assist-control, IMV, SIMV and their characteristics. - Factors to consider when selecting initial settings like rate, pressures, and tidal volumes. - How to adjust settings to impact oxygenation and ventilation. - Potential problems that can arise with mechanical ventilation.











































































