Downloaded 27 times
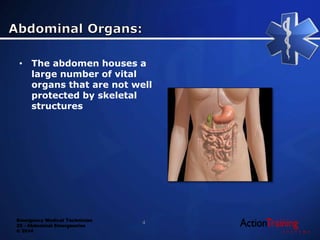

This document discusses abdominal emergencies that EMTs may encounter, including injuries, acute distress, and diseases that can affect the abdomen. It covers assessing patients with abdominal pain, identifying potential causes, managing trauma injuries, and providing emergency care, with a focus on stabilizing vital signs, controlling bleeding, and preparing patients for transport. Abdominal emergencies require prompt response due to the risk of shock if internal organs are damaged.























































































