Download to read offline




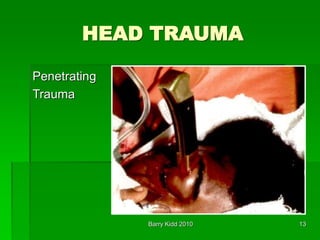









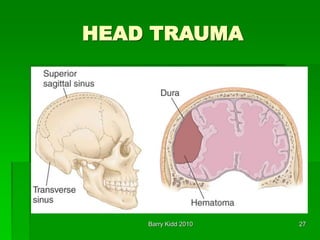


















This document discusses head trauma, including: - The anatomy of the head and brain and types of injuries like concussions, contusions, hematomas. - Primary and secondary brain injuries, with primary occurring immediately from force and secondary developing over hours from hypoxia or decreased blood flow. - Assessment of head injury patients including neurological exam signs like anisocoria and posturing that indicate increased intracranial pressure. - Management focuses on airway control, preventing hypotension, limiting agitation to reduce intracranial pressure, and treating cerebral herniation syndrome aggressively.









































![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250319190324-4867f9fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250318200004-e6284666-thumbnail.jpg?width=640&height=640&fit=bounds)












































