Downloaded 13 times

![references
• An, Y. H., & Friedman, R. J. (2000). Multidirectional instability of the GHJ Jt. The Orthopedic Clinics of North America, 31(2), 275–285.
• Barden, J. M., Balyk, R., Raso, V. J., Moreau, M., & Bagnall, K. (2005). Atypical Sh M activation in multidirectional instability. Clinical Neurophysiology: Official Journal of the International Federation of Clinical
Neurophysiology, 116(8), 1846–1857. http://doi.org/10.1016/j.clinph.2005.04.019
• Barrett, C. (2015). The clinical physiotherapy assessment of non-traumatic Sh instability. Sh & Elbow, 7(1), 60–71. http://doi.org/10.1177/1758573214548934
• Bateman, M., Smith, B. E., Osborne, S. E., & Wilkes, S. R. (2015). Physiotherapy Tx for atraumatic recurrent Sh instability: early results of a specific exercise protocol using pathology-specific outcome measures. Sh &
Elbow, 1758573215592266. http://doi.org/10.1177/1758573215592266
• Burkhead, W. Z., & Rockwood, C. A. (1992). Tx of instability of the Sh with an exercise program. The Journal of Bone & Jt Sx. American Volume, 74(6), 890–896.
• Illyés, Á., Kiss, J., & Kiss, R. M. (2009). Electromyographic analysis during pull, forward punch, elevation & overhead throw after conservative Tx or capsular shift at patient with multidirectional Sh Jt instability. Journal of
Electromyography & Kinesiology, 19(6), e438–e447. http://doi.org/10.1016/j.jelekin.2008.09.008
• Kiss, J., Damrel, D., Mackie, A., Neumann, L., & Wallace, W. A. (2001). Non-operative Tx of multidirectional Sh instability. International Orthopaedics, 24(6), 354–357.
• Labriola, J. E., Lee, T. Q., Debski, R. E., & McMahon, P. J. (2005). Stability & instability of the GHJ Jt: The role of Sh Ms. Journal of Sh & Elbow Sx, 14(1, Supplement), S32–S38. http://doi.org/10.1016/j.jse.2004.09.014
• Longo, U. G., Rizzello, G., Loppini, M., Locher, J., Buchmann, S., Maffulli, N., & Denaro, V. (2015). Multidirectional Instability of the Sh: A Systematic Review. Arthroscopy: The Journal of Arthroscopic & Related Sx, 31(12),
2431–2443. http://doi.org/10.1016/j.arthro.2015.06.006
• Merolla, G., Cerciello, S., Chillemi, C., Paladini, P., Santis, E. D., & Porcellini, G. (2015). Multidirectional instability of the Sh: biomechanics, clinical presentation, & Tx strategies. European Journal of Orthopaedic Sx &
Traumatology, 25(6), 975–985. http://doi.org/10.1007/s00590-015-1606-5
• Misamore, G. W., Sallay, P. I., & Didelot, W. (2005). A longitudinal study of Pts with multidirectional instability of the Sh with seven- to ten-year follow-up. Journal of Sh & Elbow Sx, 14(5), 466–470.
http://doi.org/10.1016/j.jse.2004.11.006
• Nyiri, P., Illyés, A., Kiss, R., & Kiss, J. (2010). Intermediate biomechanical analysis of the effect of physiotherapy only compared with capsular shift & physiotherapy in multidirectional Sh instability. Journal of Sh & Elbow
Sx / American Sh & Elbow +-Surgeons ... [et Al.], 19(6), 802–813. http://doi.org/10.1016/j.jse.2010.05.008
• Struyf, F., Nijs, J., Baeyens, J.-P., Mottram, S., & Meeusen, R. (2011). Scapular positioning & movement in unimpaired Shs, Sh impingement syndrome, & GHJ instability. Sc&inavian Journal of Medicine & Science in
Sports, 21(3), 352–358. http://doi.org/10.1111/j.1600-0838.2010.01274.x
• Warby, S. A., Pizzari, T., Ford, J. J., Hahne, A. J., & Watson, L. (2015). Exercise-based management versus Sx for multidirectional instability of the GHJ Jt: a systematic review. British Journal of Sports Medicine, bjsports–
2015–094970. http://doi.org/10.1136/bjsports-2015-094970
• Warner, J. J. P. (n.d.). Role of Proprioception in Pathoetiology of Sh Instabil... : Clinical Orthopaedics & Related Research. Retrieved May 26, 2015, from
http://journals.lww.com/corr/Fulltext/1996/09000/Role_of_Proprioception_in_Pathoetiology_of.5.aspx](https://image.slidesharecdn.com/macphysioprinciplesandmanagemntmdi-160601111531/85/Atraumatic-MDI-Physiotherapy-Principles-and-Management-36-320.jpg)

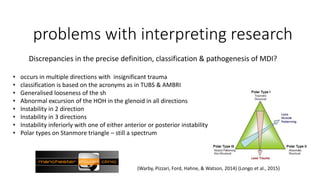
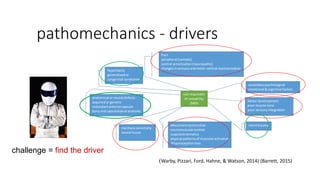
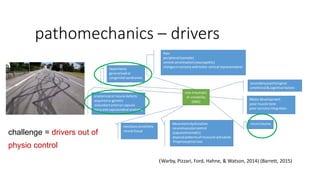
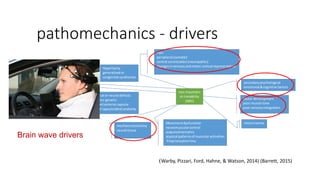
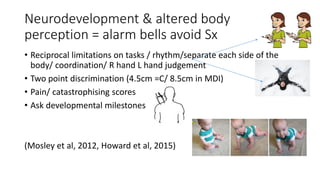
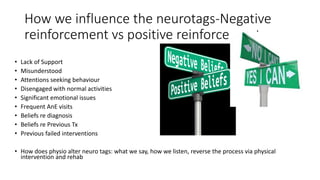
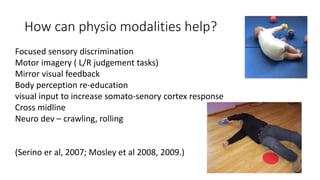
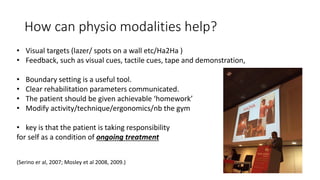
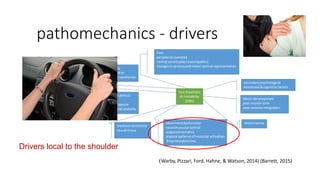
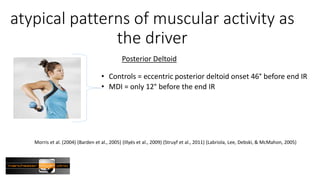
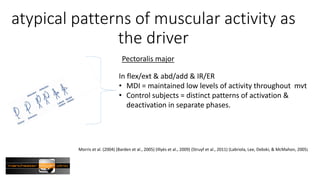
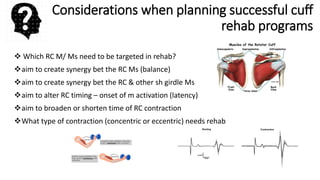
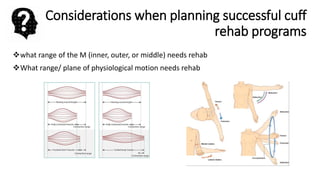
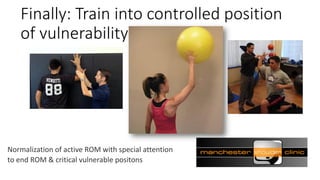
Physiotherapy management of multidirectional instability (MDI) of the shoulder is complex due to various drivers of the condition. Research on MDI has been difficult to interpret due to inconsistent definitions, heterogeneous populations, lack of standardization, and insensitive outcome measures across studies. Physiotherapy aims to address drivers both local to the shoulder like atypical muscle activation patterns and scapular kinematics, as well as central nervous system drivers involving cortical reorganization. Rehabilitation focuses on normalizing range of motion, improving neuromuscular control, and training into positions of vulnerability using modalities that target specific muscles individually and create synergies between muscles.





















































































