Download to read offline
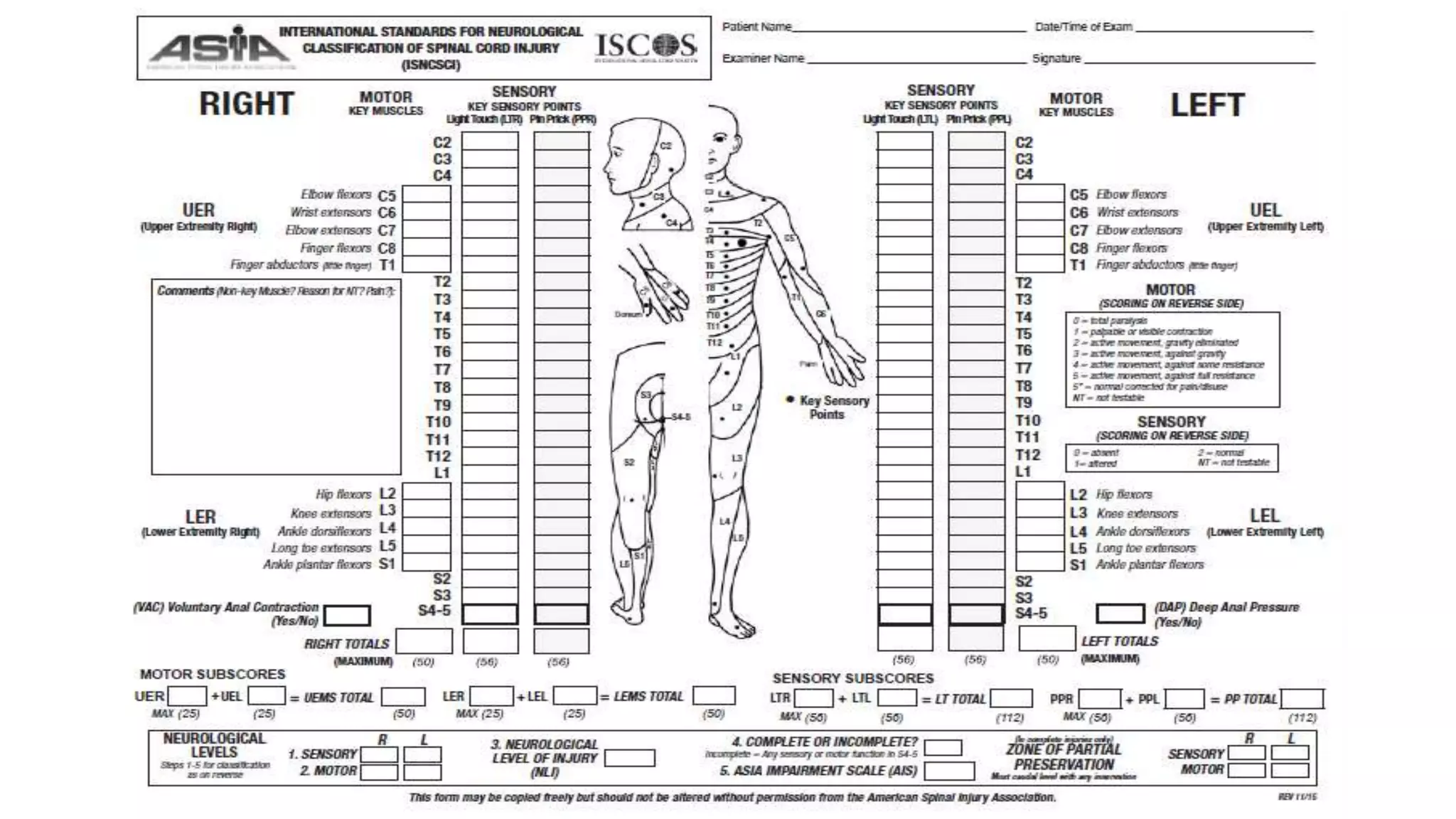

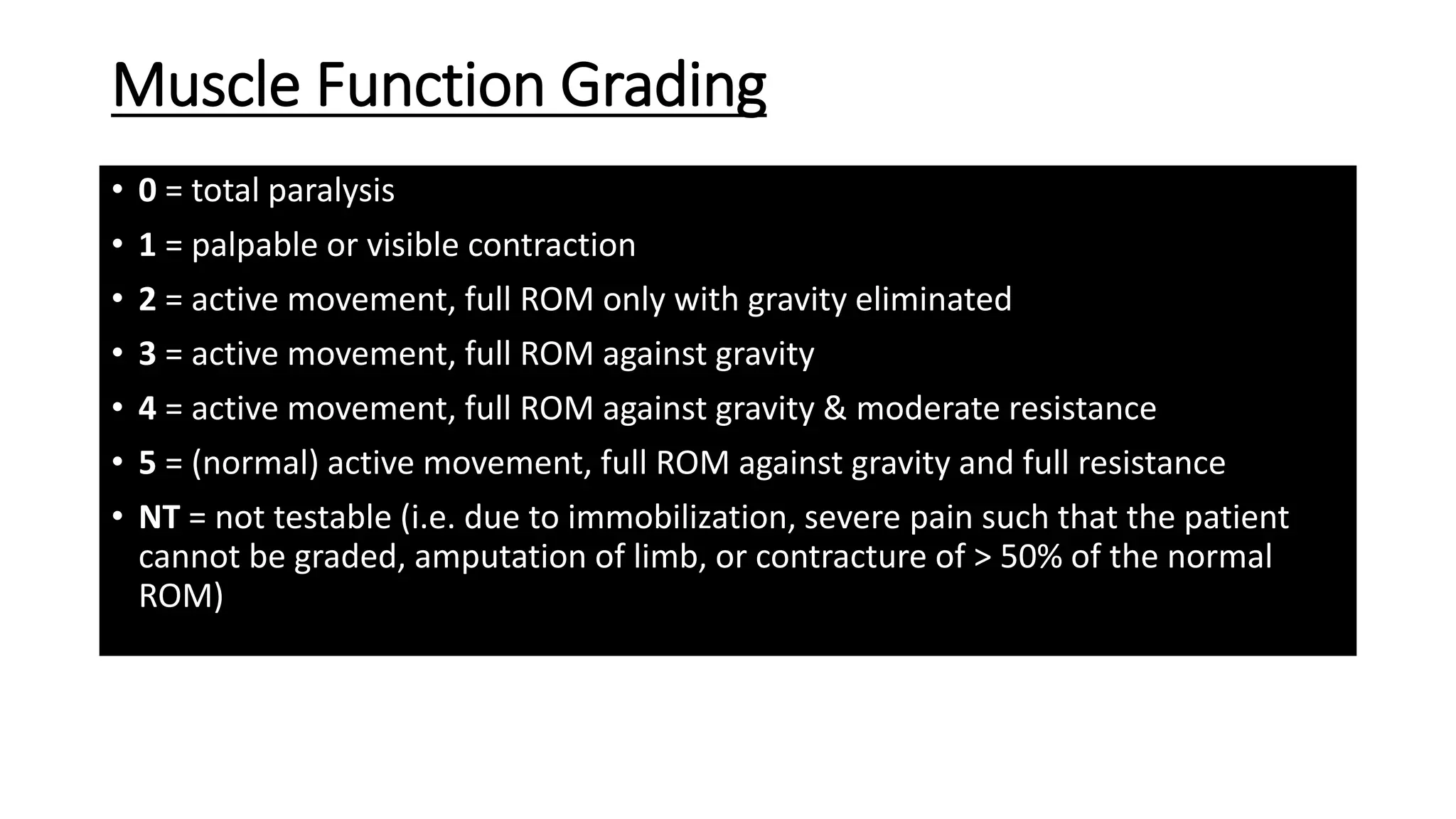

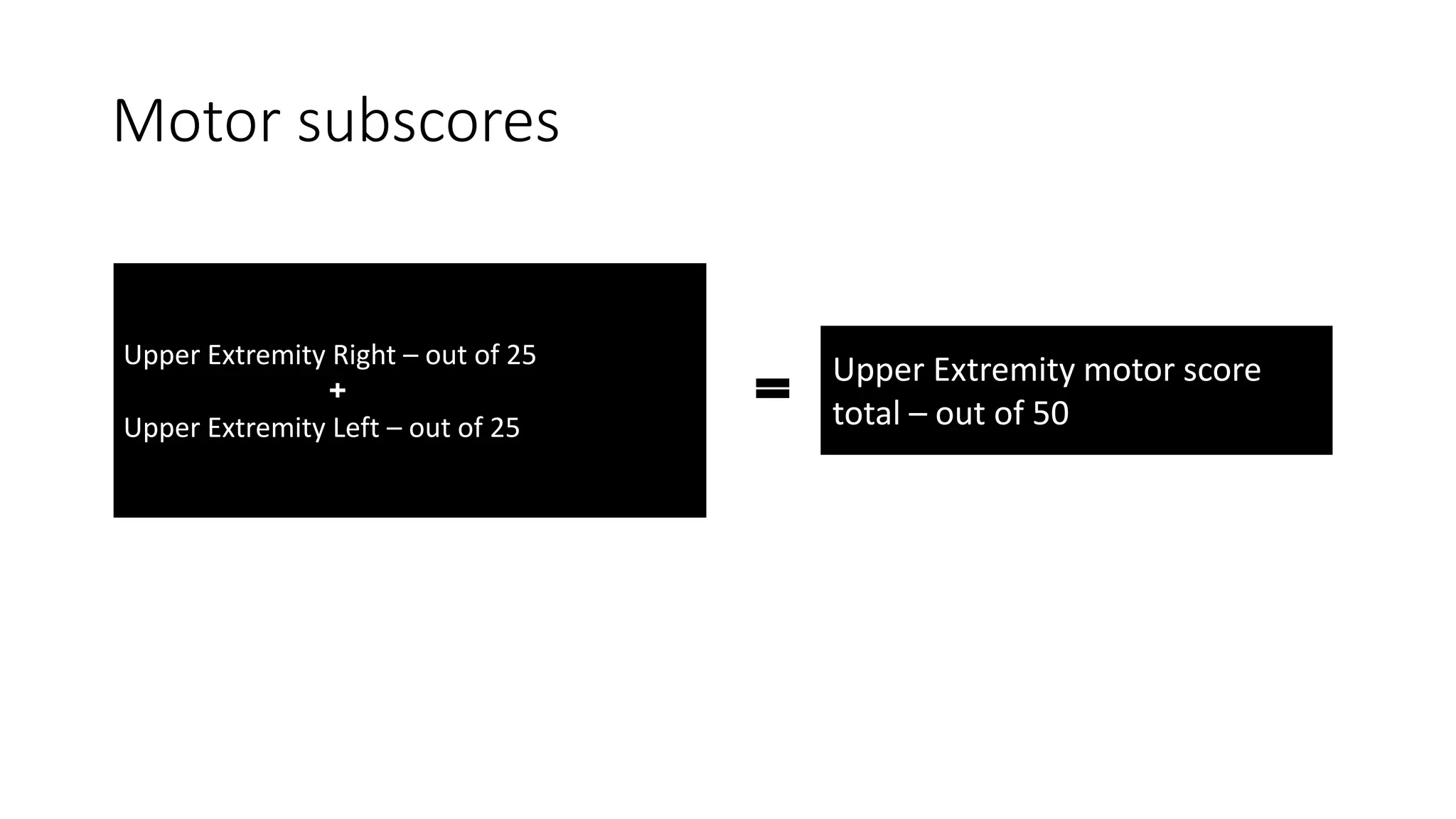
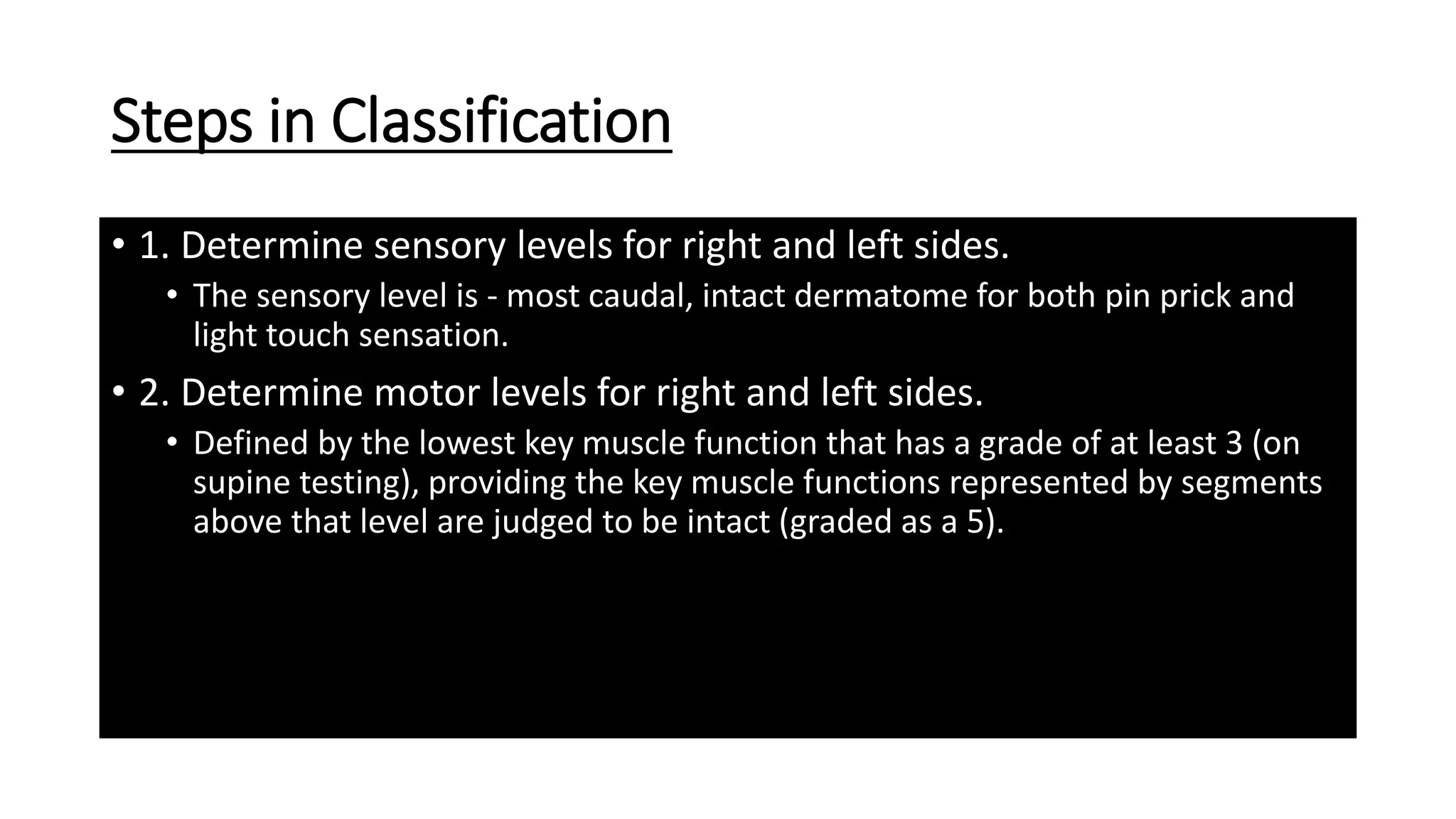
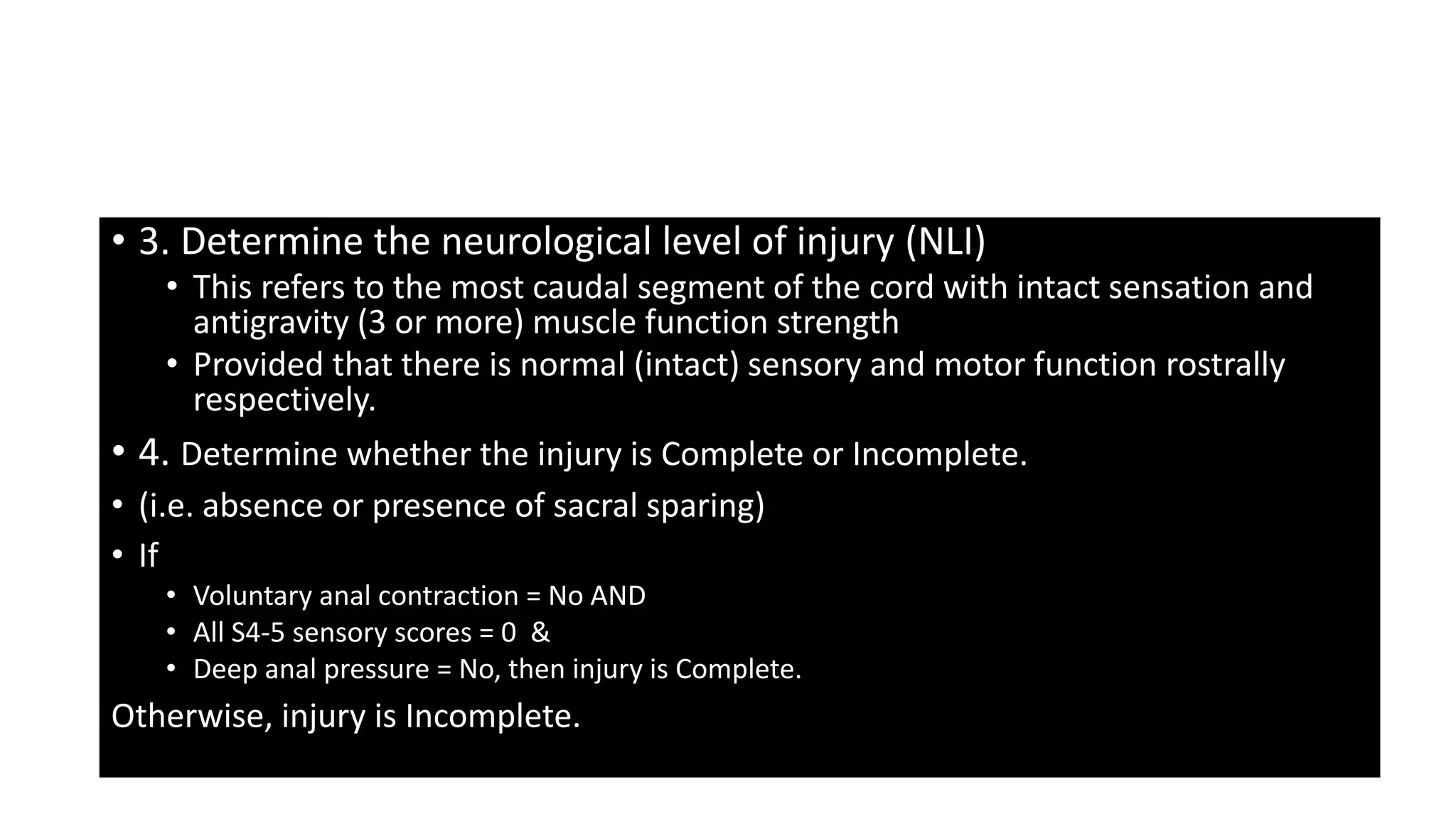
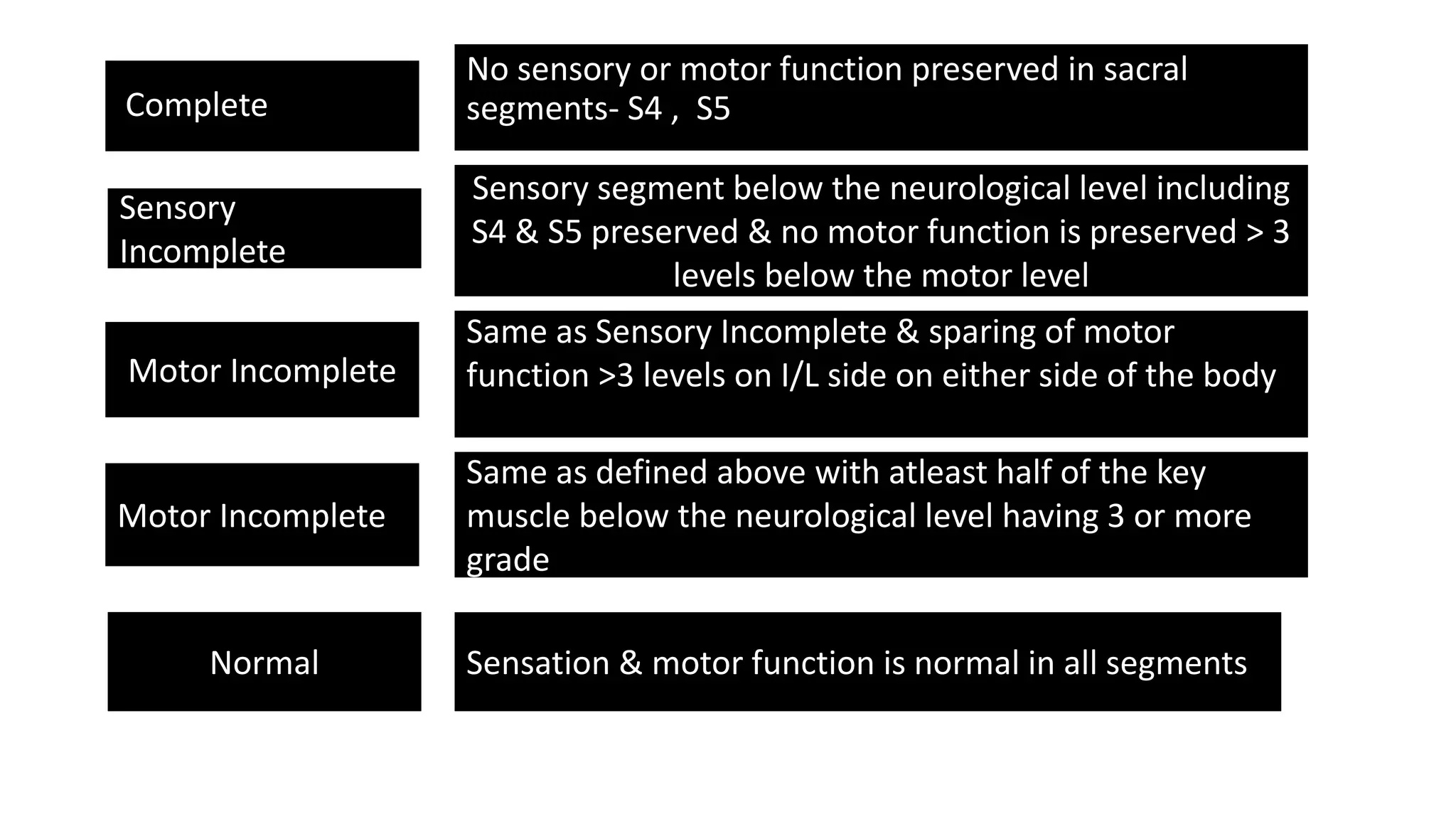

The document provides information on assessing spinal cord injuries, including key muscles associated with different spinal cord levels, grading scales for muscle function and sensory ability, how to evaluate motor and sensory subscores, and the steps to classify a spinal cord injury as complete or incomplete. It defines a complete injury as having no sensory or motor function preserved in sacral segments S4-S5, while an incomplete injury has some sensory or motor function spared below the neurological level.























































































