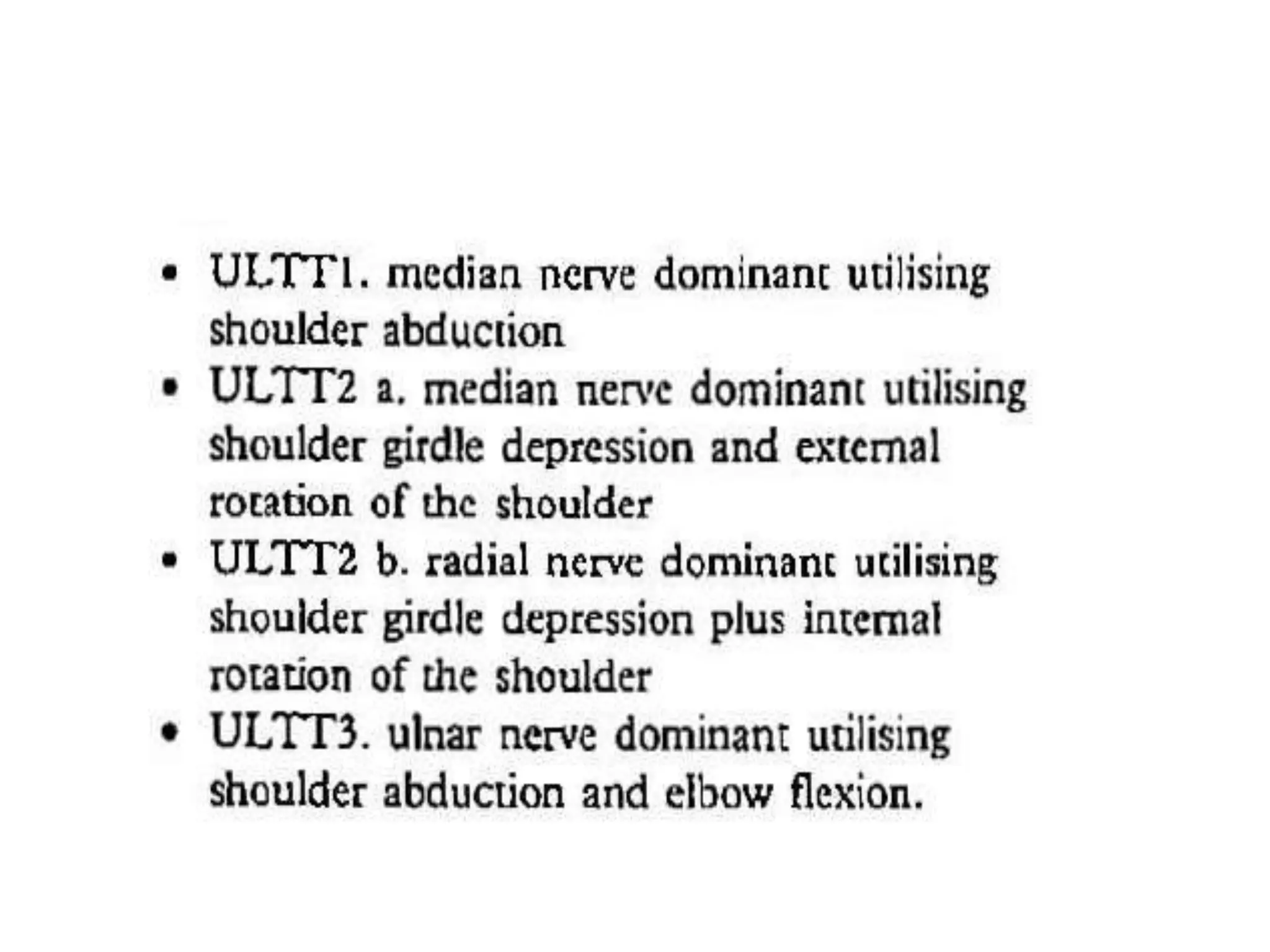
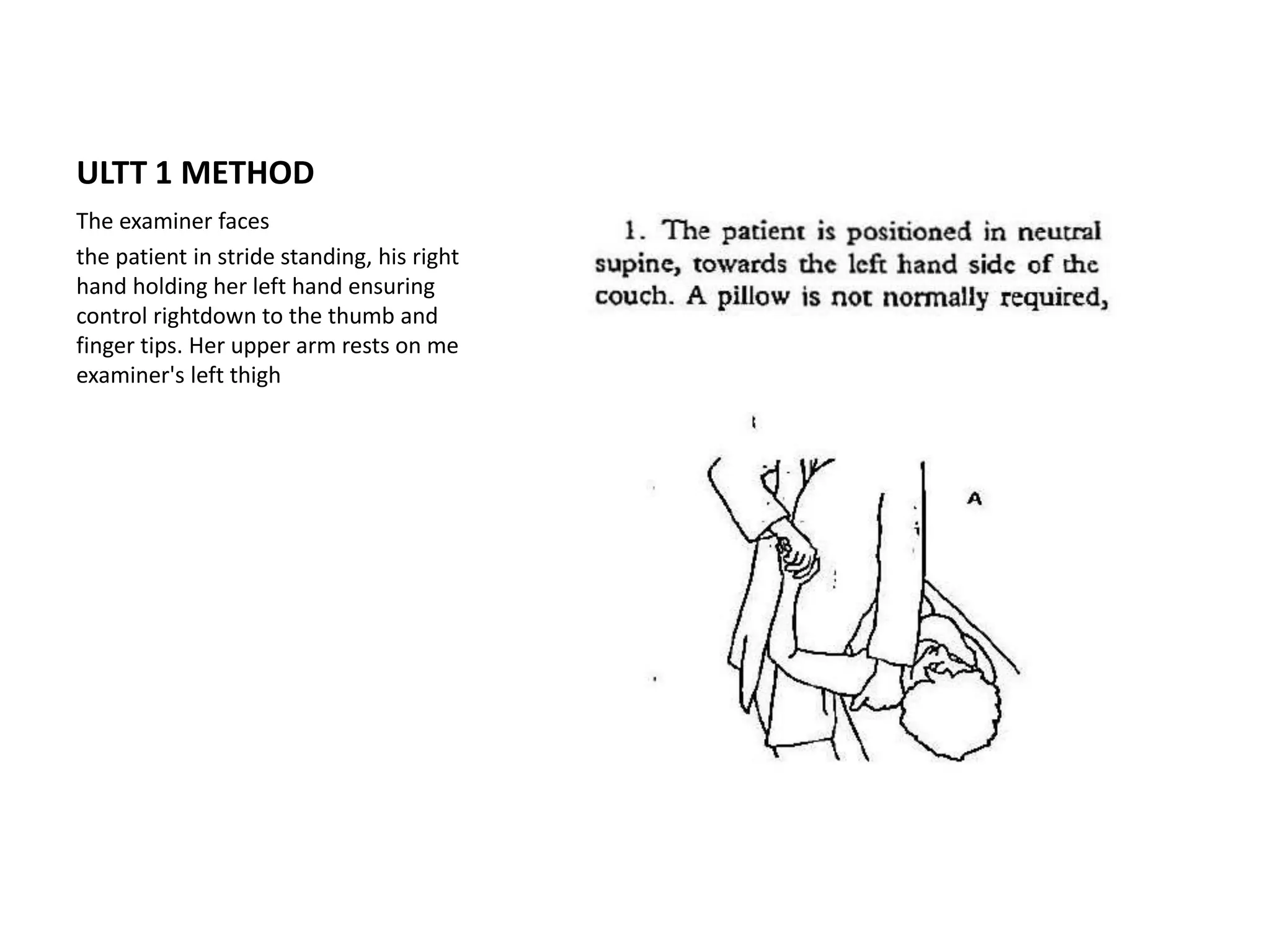
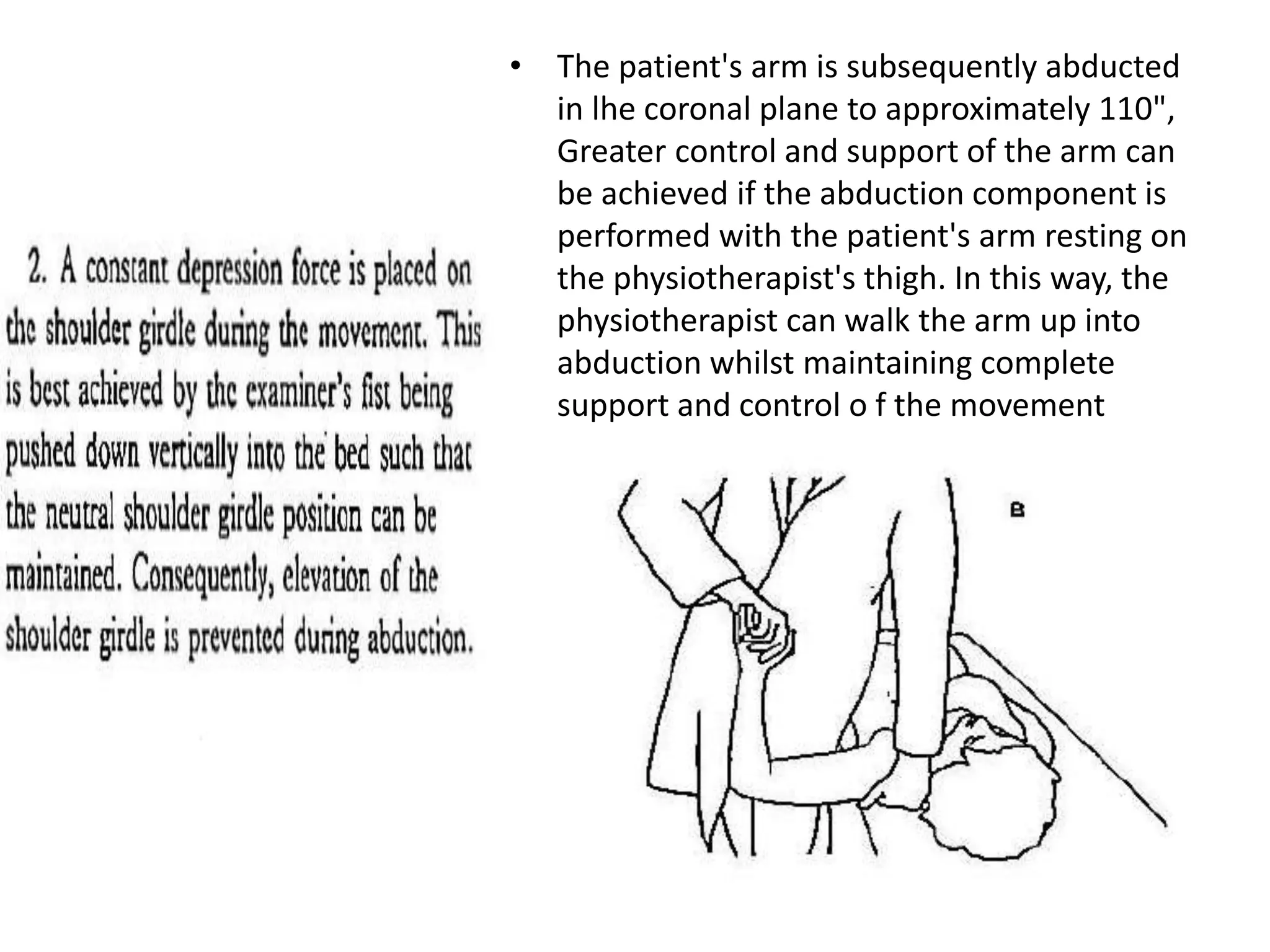
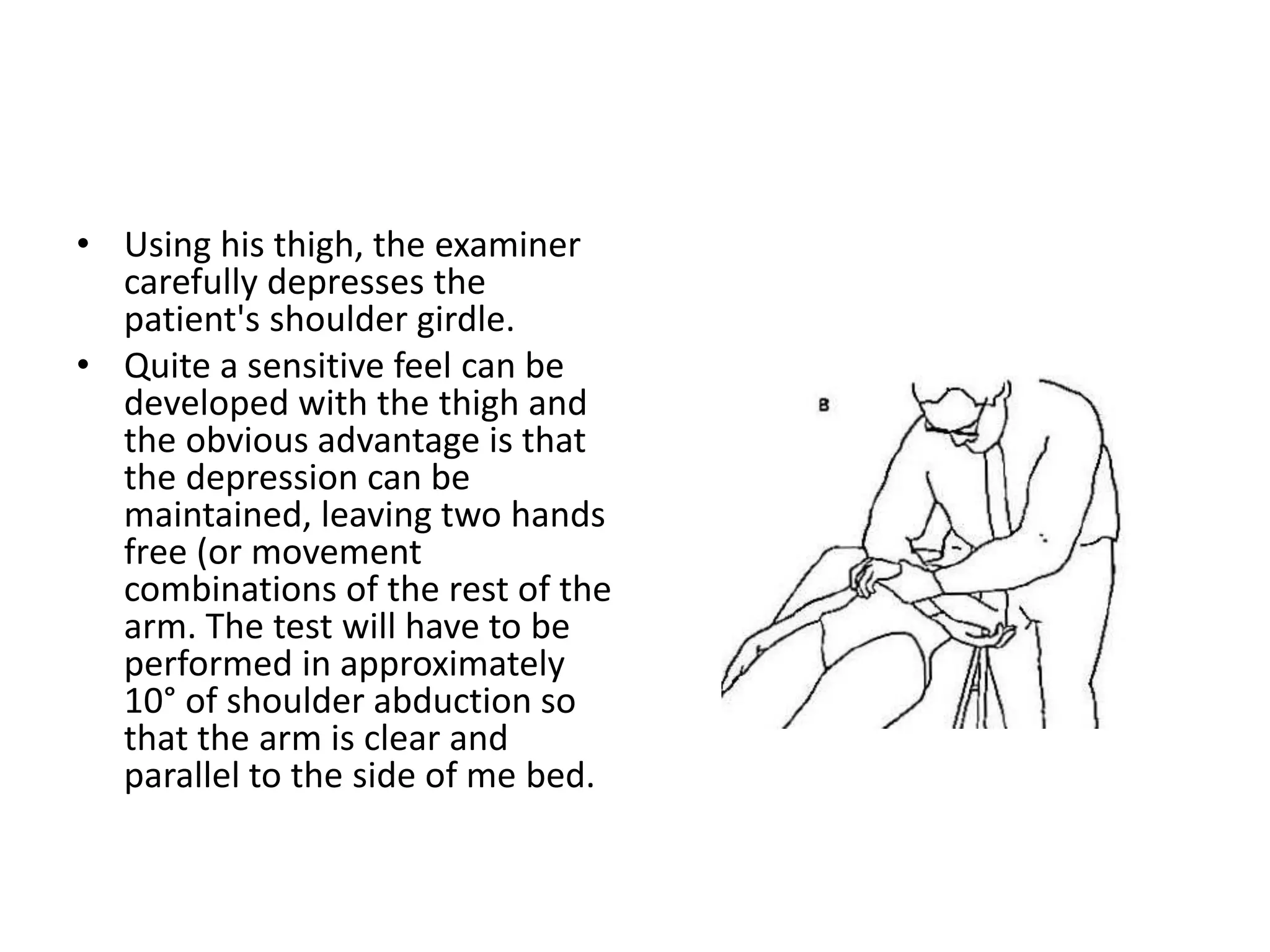
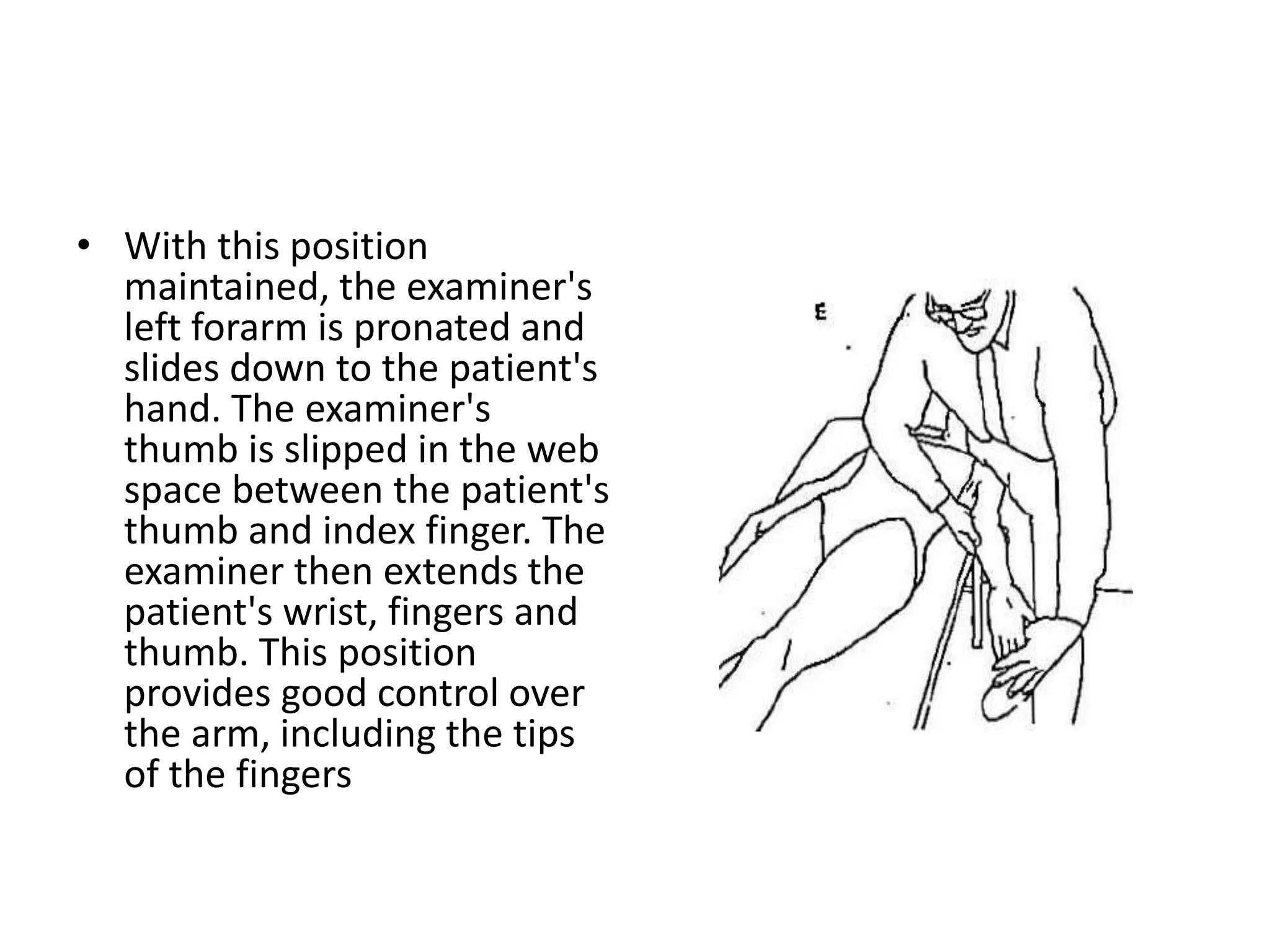
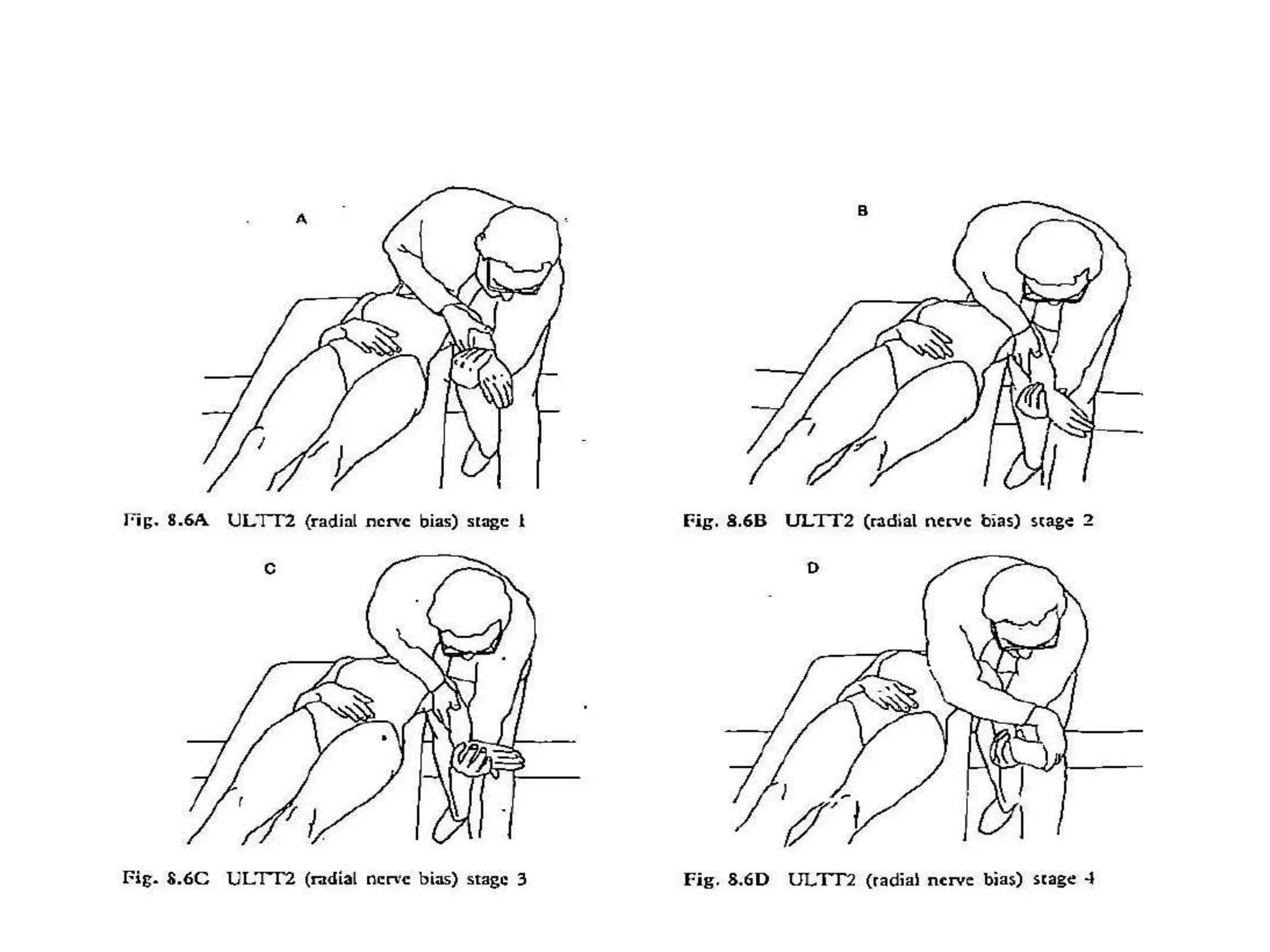
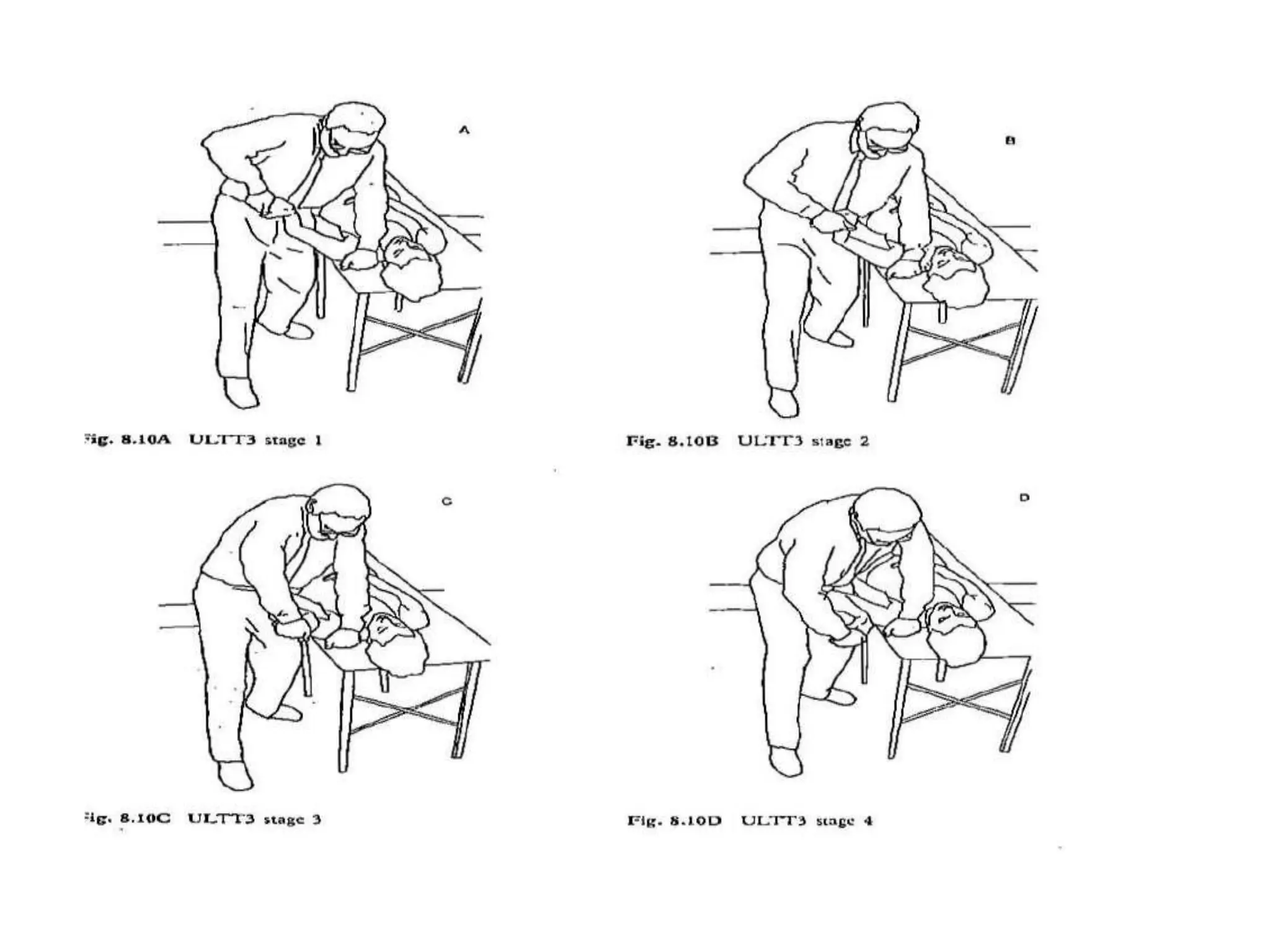
This document describes three upper limb tension tests (ULTT1, ULTT2, ULTT3) used to assess the cervical spine and brachial plexus. ULTT1 involves abducting, supinating, and laterally rotating the shoulder while extending the elbow and wrist. ULTT2 adds shoulder depression while extending the elbow and laterally rotating the arm. ULTT3 (ulnar nerve bias) assesses the cubital tunnel by having the patient flex their elbow while the examiner controls their hand and arm. Precautions are described and variations discussed, including assessing different angles of abduction. The tests aim to isolate tensions and identify symptoms to determine involved structures.