Downloaded 137 times
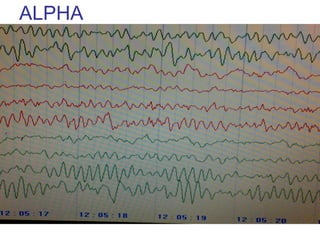

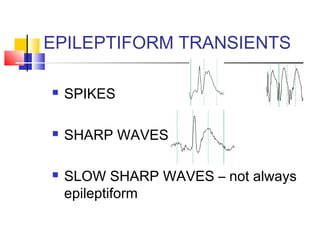
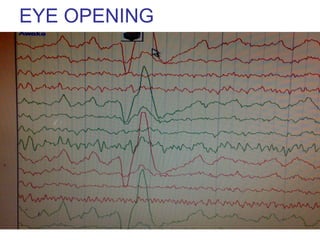
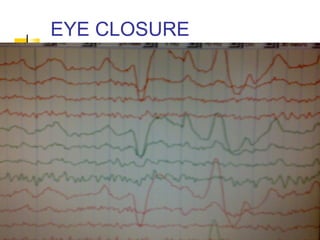
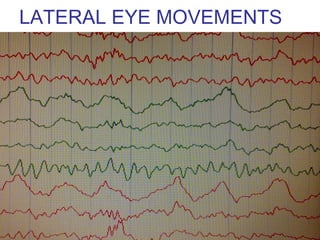
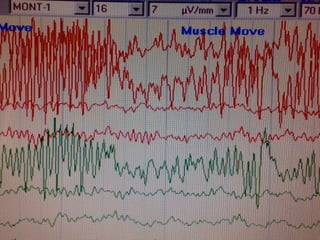
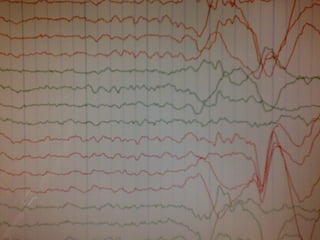
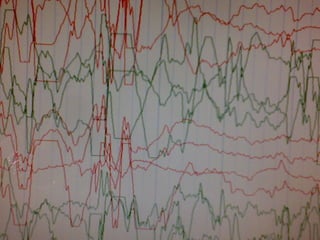
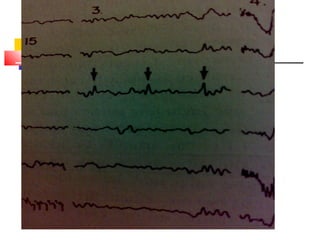
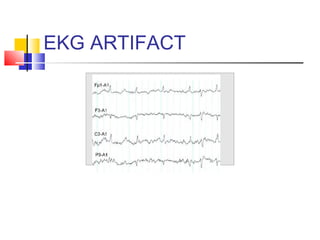
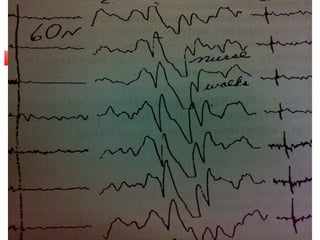
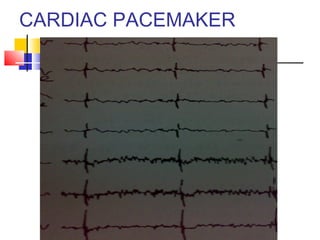

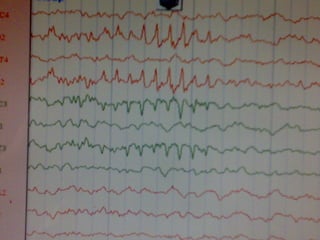
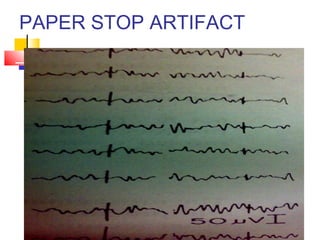
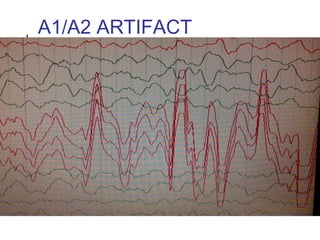
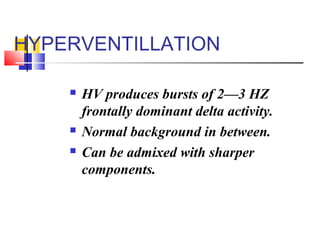
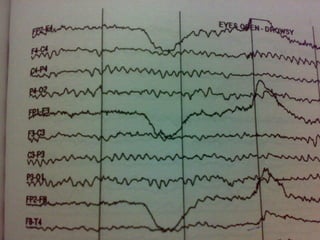



This document discusses artifacts and normal variants that may appear on EEG recordings. It describes various types of artifacts that can originate from patient physiology like eye movements, muscle activity, and heartbeats. It also discusses artifacts from external interference and equipment issues. Normal variants are described like alpha rhythm, sleep transients, and frontal rhythms seen in drowsiness that should not be mistaken for epileptiform activity. The document provides details on identifying features of each artifact and variant to differentiate them from cerebral abnormalities.













































































