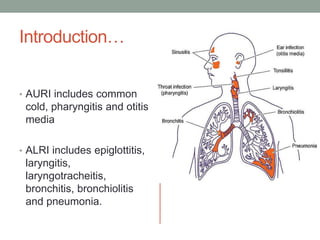
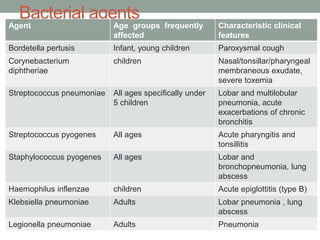
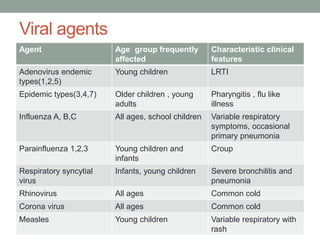
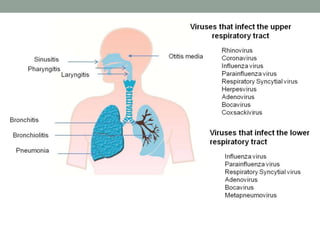
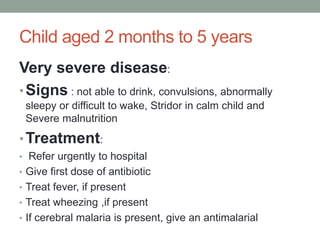
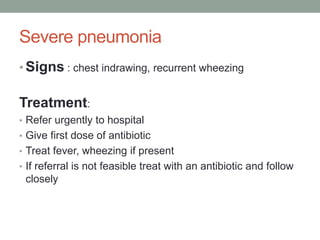
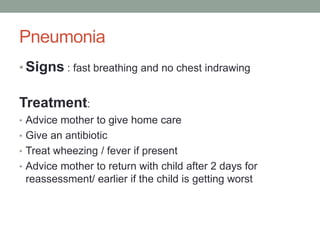
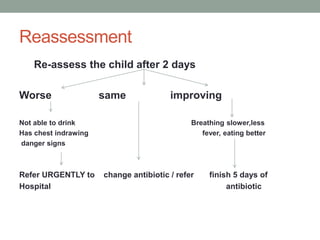
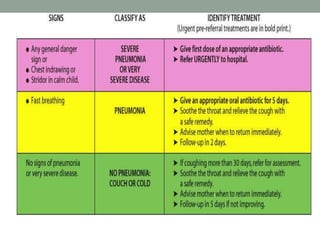
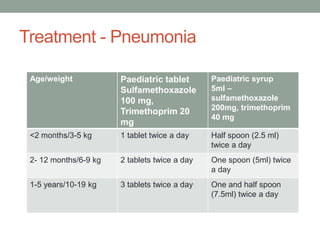
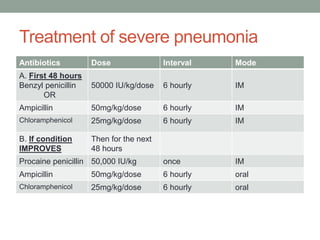
This document discusses acute respiratory infections (ARI), including their causes, transmission, clinical assessment, classification, treatment, and prevention. It describes the different bacterial and viral agents that can cause ARIs. Clinical assessment involves examining symptoms, breathing rate, chest indrawing, wheezing, and malnutrition. ARIs are classified based on severity and treated with antibiotics or symptomatic care. Prevention focuses on improved living conditions, nutrition, immunization including measles vaccine, Hib vaccine, and pneumococcal pneumonia vaccine.