Downloaded 96 times

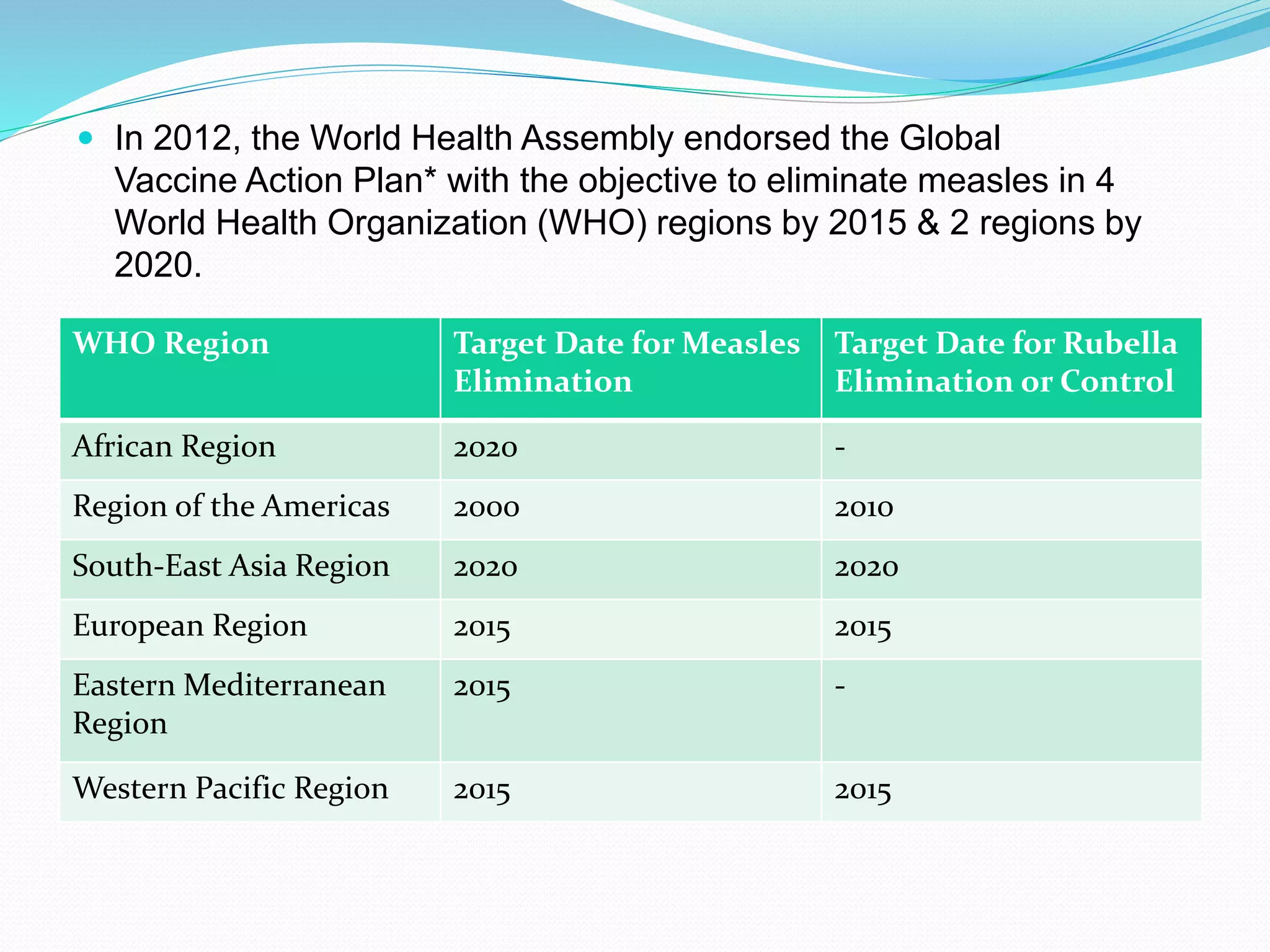






This document discusses four infectious diseases: smallpox, chickenpox, rubella, and measles. It provides details on the causative agents, transmission, epidemiology, and global status of each disease. For smallpox, it notes it has been eradicated worldwide since the last case in 1977. For chickenpox and measles, introduction of vaccines has led to a significant reduction in deaths. Rubella cases also occur worldwide but vaccination aims to eliminate it in several WHO regions by targeted dates. Overall, the document outlines the key facts about these four viral diseases.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






