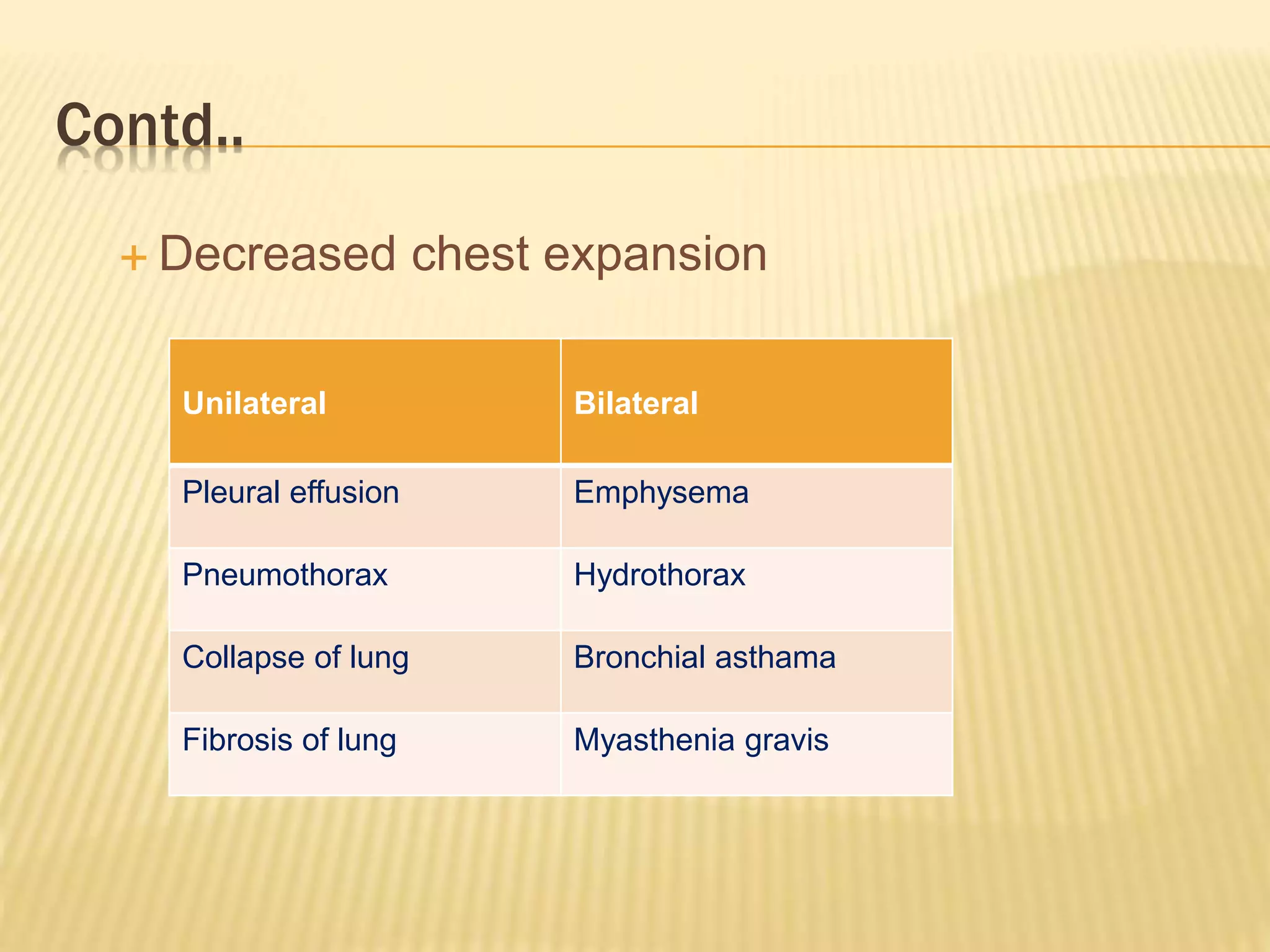
The document provides details on inspecting and examining the chest. It discusses assessing the shape of the chest and noting any deformities. It describes examining the movement of the chest on respiration and listening for breath sounds such as vesicular, bronchial, crackles, rhonchi and wheeze. Specific techniques for percussion and auscultation of the chest are outlined. Common abnormalities and associated conditions are mentioned.












































































































![chapter 4 Physical diagnosis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicaldiagnosisautosaved-250416123318-d2df54aa-thumbnail.jpg?width=640&height=640&fit=bounds)







![Respiratory System PE-1 [Autosaved].ppttiteciex](https://cdn.slidesharecdn.com/ss_thumbnails/respiratorysystempe-1autosaved-250113170401-72d39633-thumbnail.jpg?width=640&height=640&fit=bounds)





















