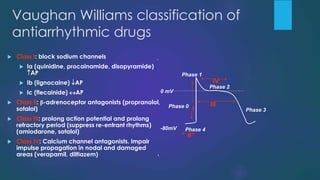
The document provides an extensive overview of antiarrhythmic agents in veterinary medicine, detailing the mechanisms of action, physiological phases of cardiac action potentials, and various types of arrhythmias. It categorizes antiarrhythmic drugs into four main classes based on the Vaughan-Williams classification, discussing specific drug examples, their indications, contraindications, and effects. The management of arrhythmias includes the use of these drugs, as well as techniques like cardiac pacemakers and catheter ablation.
![etiology
Ischemia/hypoxemia
Imbalance of the parasympathetic & sympathetic
branches of the ANS
Serum electrolyte imbalance[K+ & Ca ++]
Activation of RAAS
Pharmacologic therapy
Inherited causes (rare)
Arrhythmia associated with acquired heart diseases viz
CHF, viral myocarditis etc
Infarction of the heart muscle](https://image.slidesharecdn.com/antiarryhtmia-140610041746-phpapp01/85/ANTIARRHYTHMIC-AGENTS-IN-VETERINARY-PRACTICE-8-320.jpg)