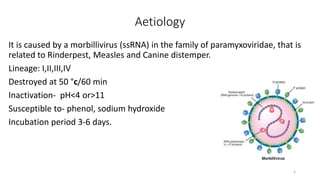
Peste des petits ruminants (PPR) is a highly contagious viral disease affecting goats and sheep, characterized by symptoms such as fever, sores, pneumonia, and potentially death. The disease, caused by a morbillivirus, has a significant mortality rate, particularly among goats, and has spread across various regions since its first description in 1940. Prevention includes strict quarantine, sanitation measures, and vaccination, while treatment remains largely supportive with no specific cure.