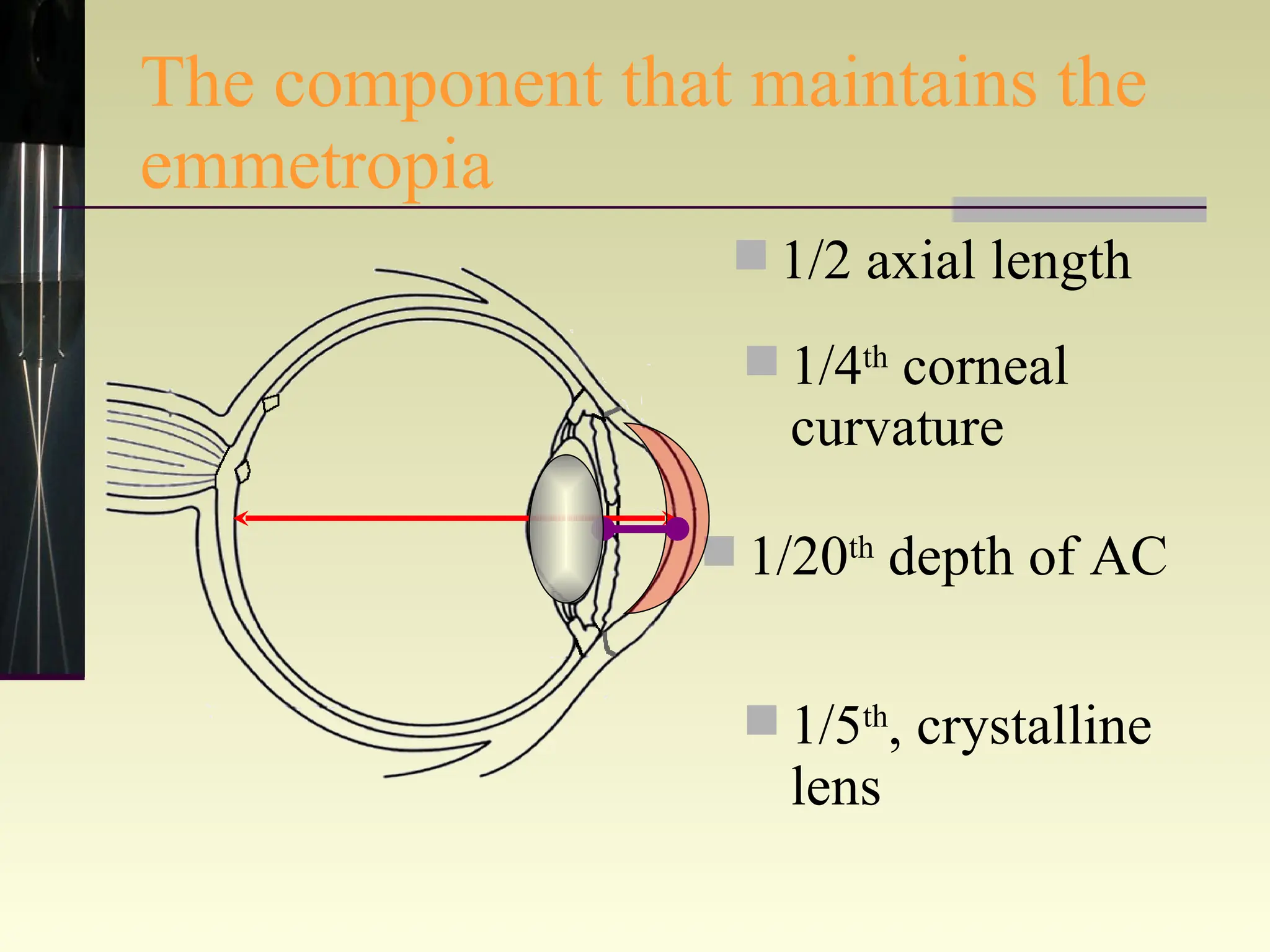
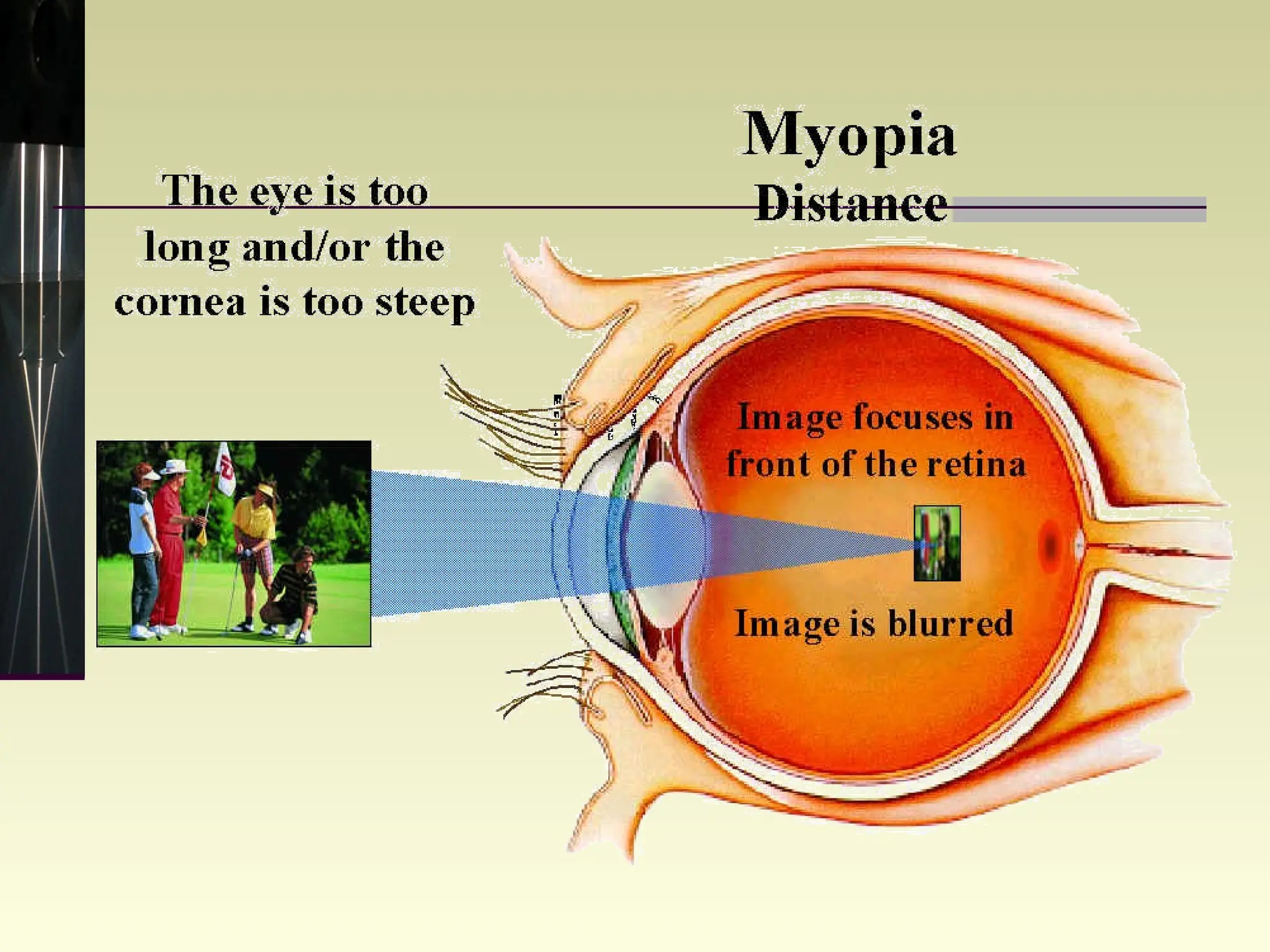
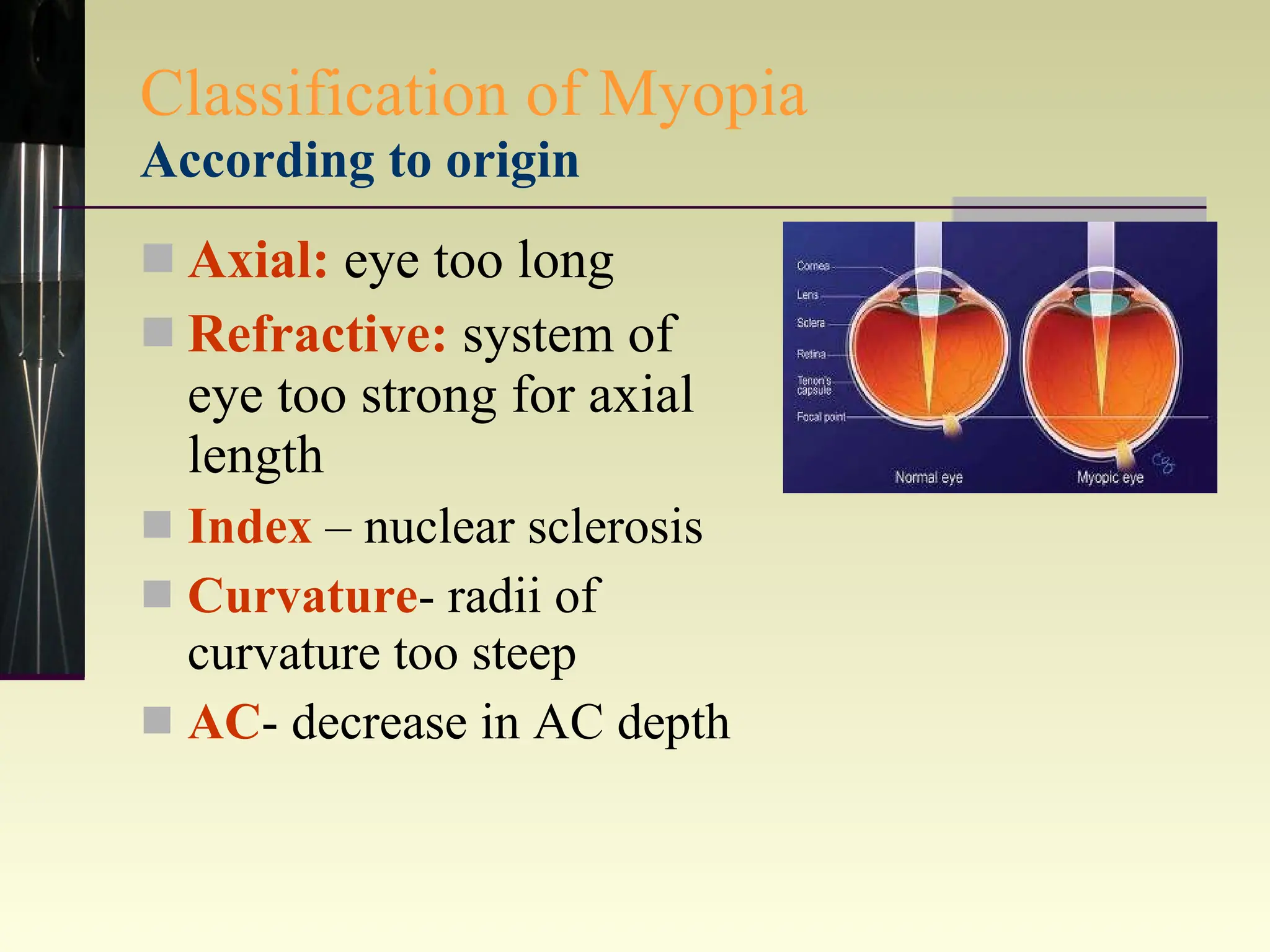
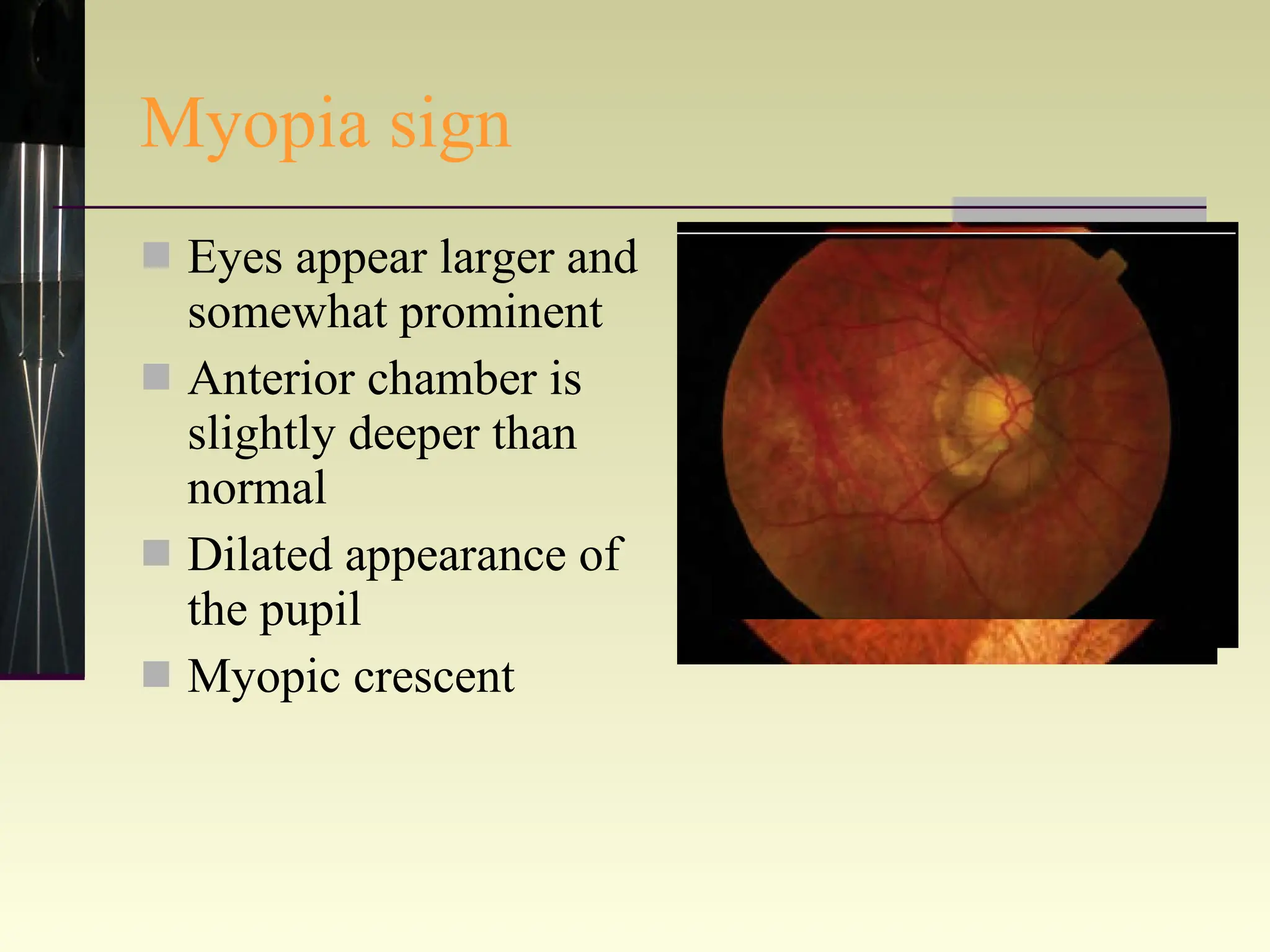
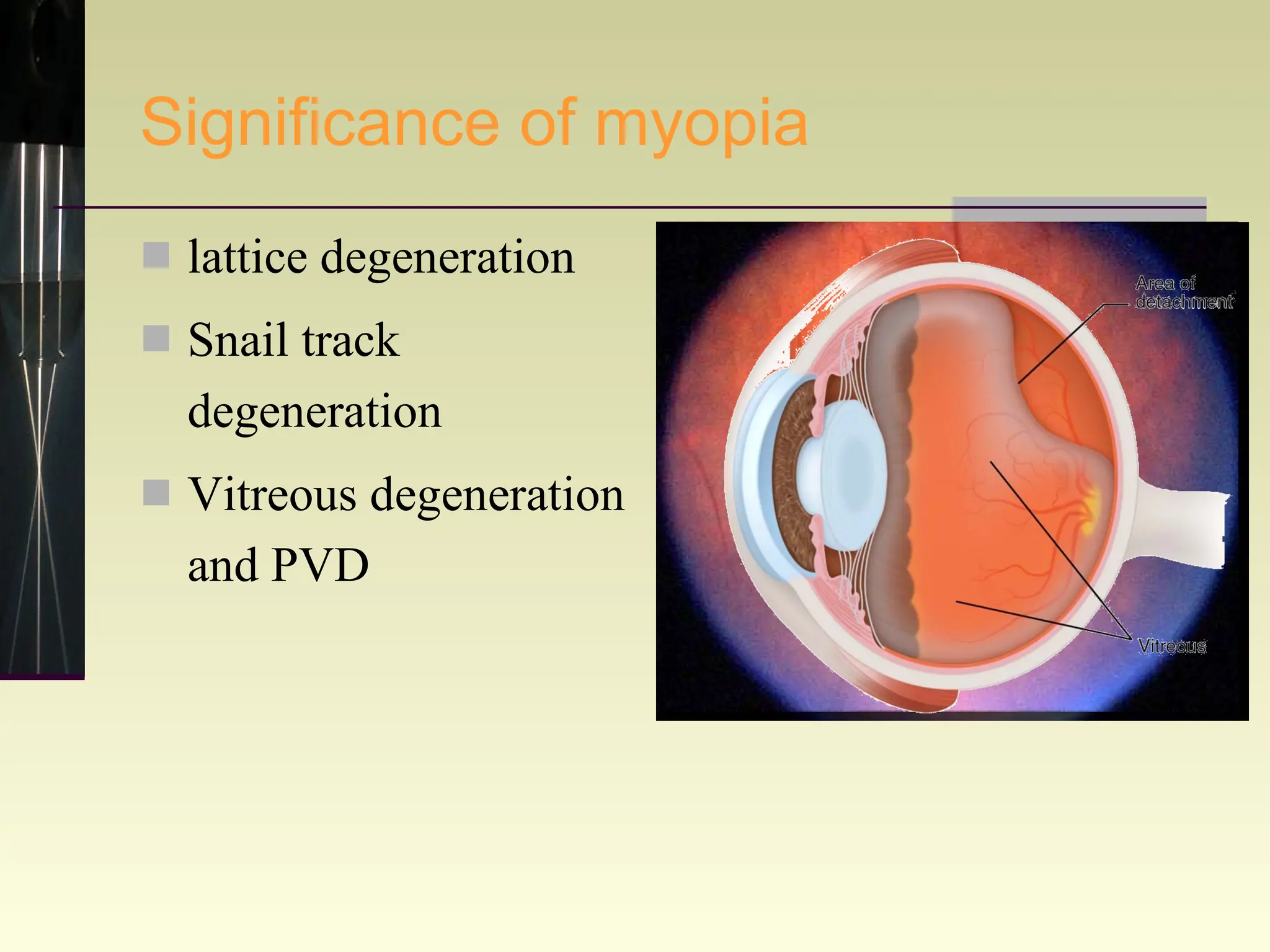
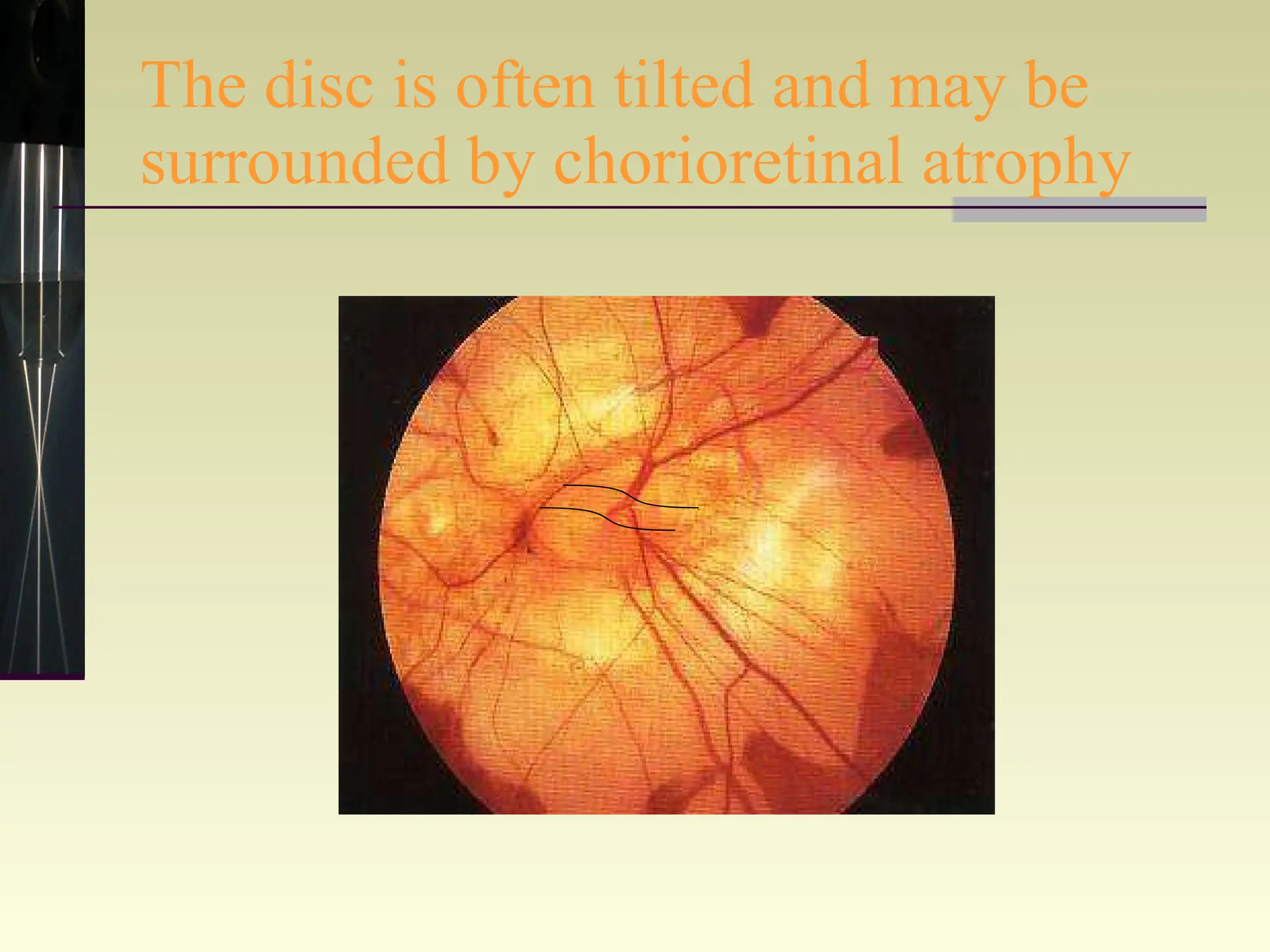

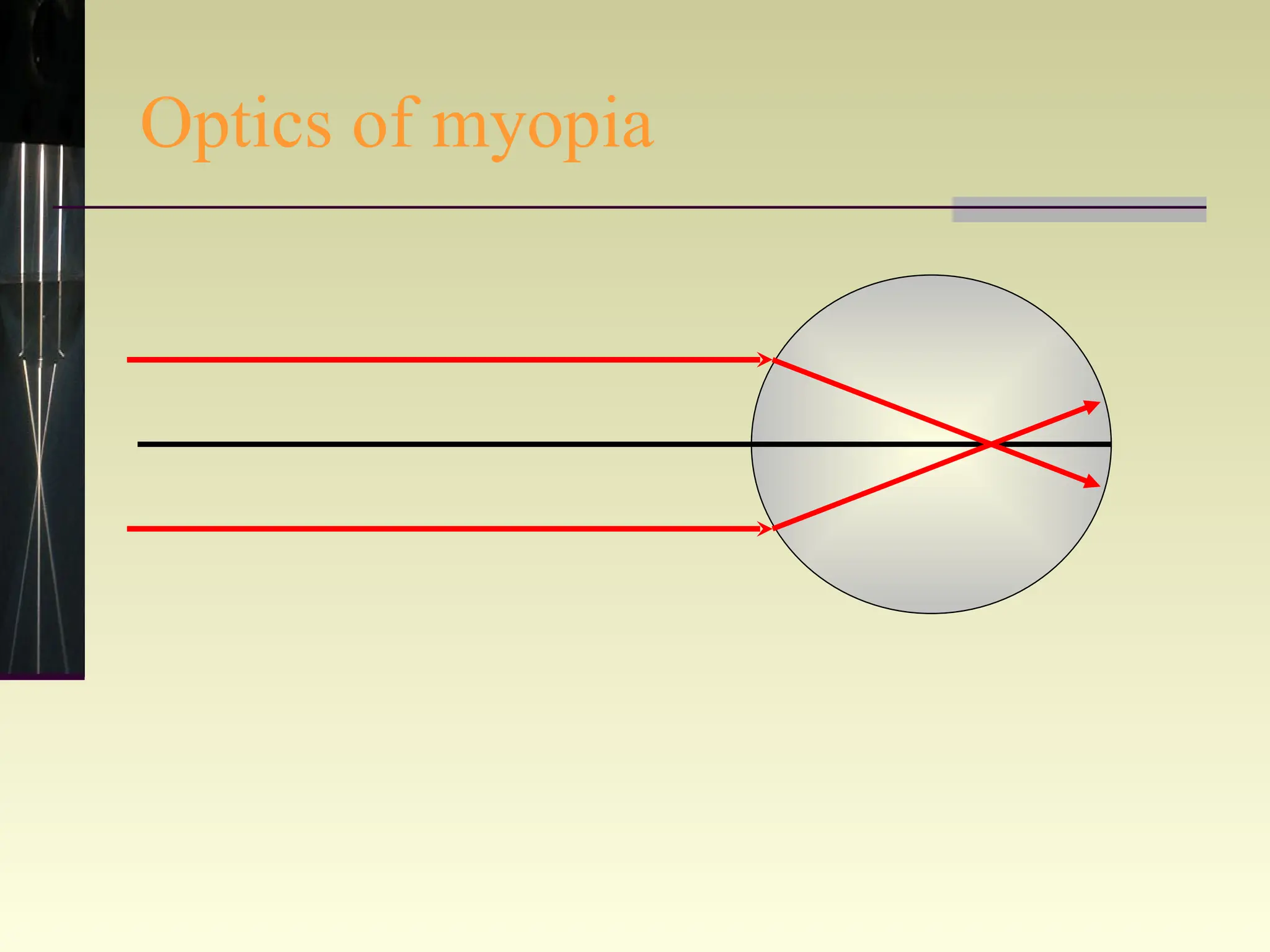
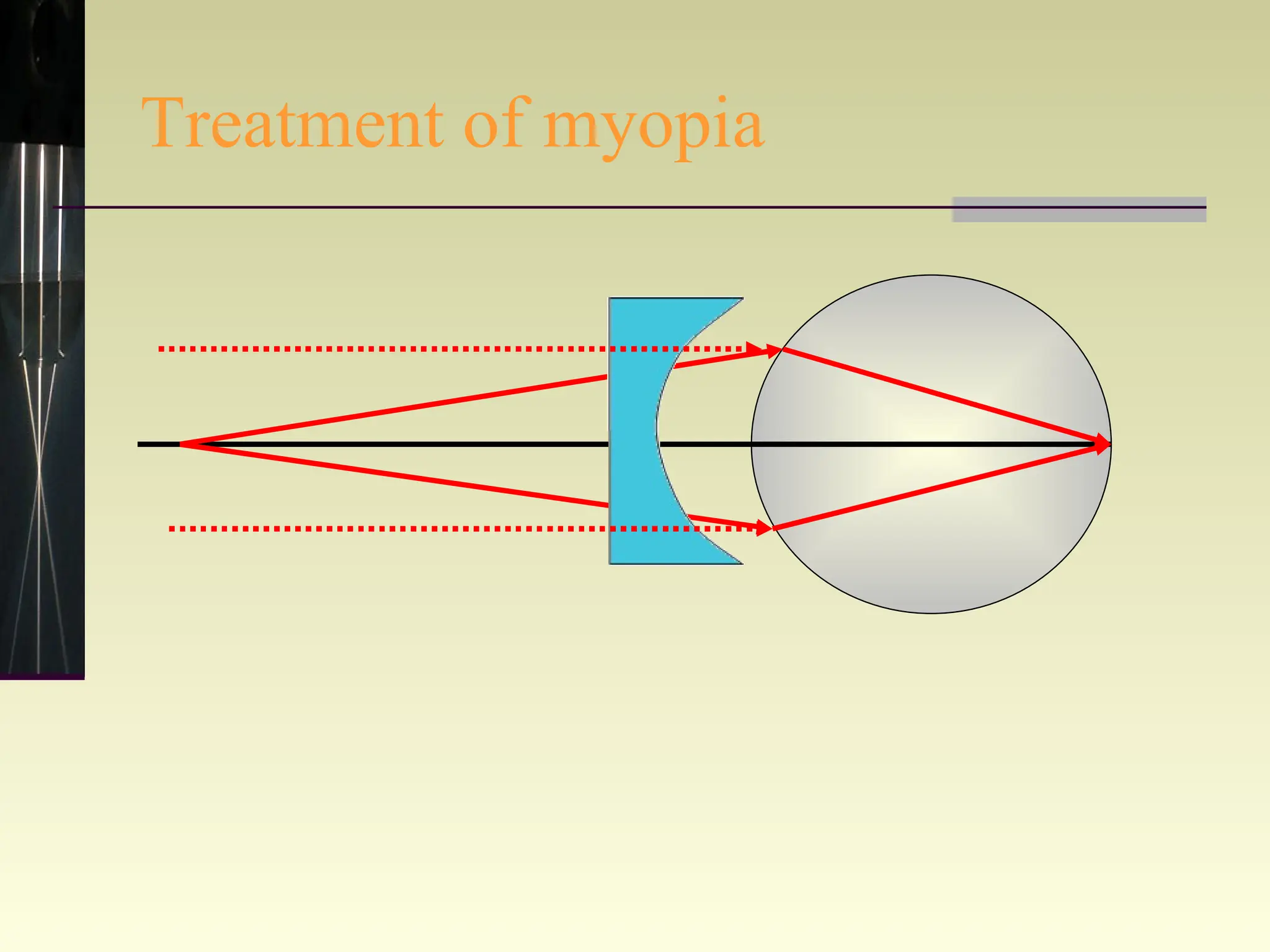
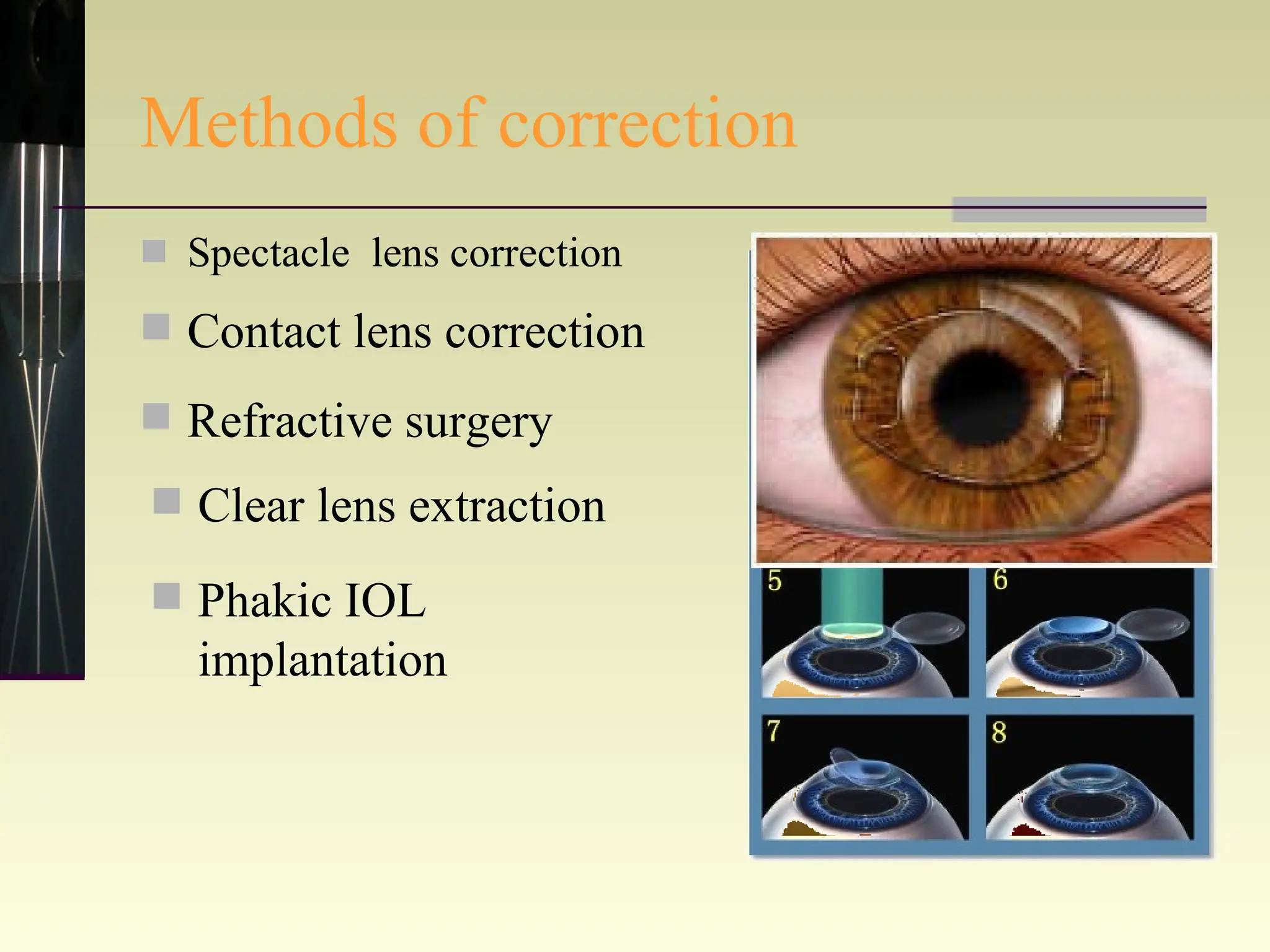
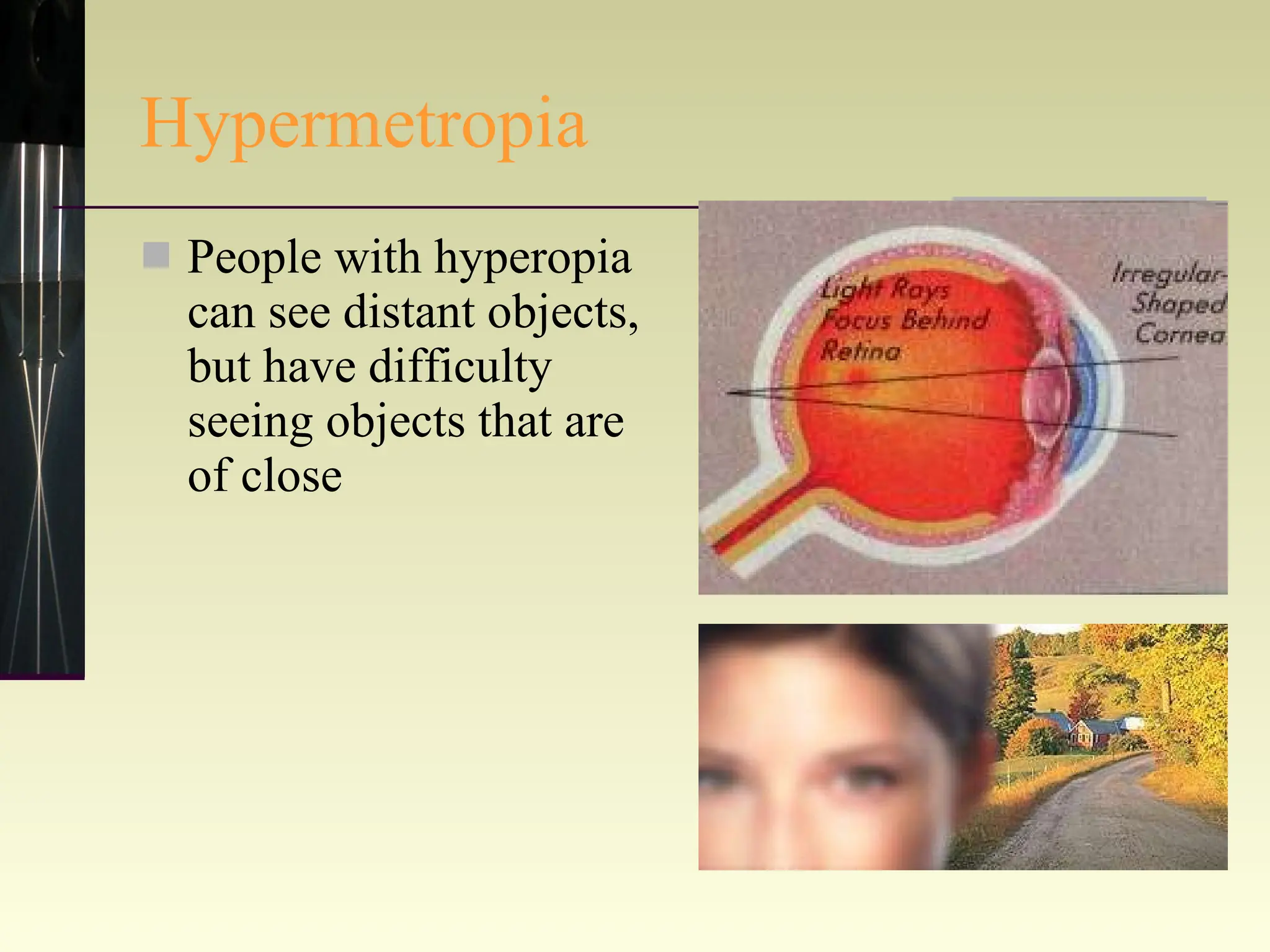
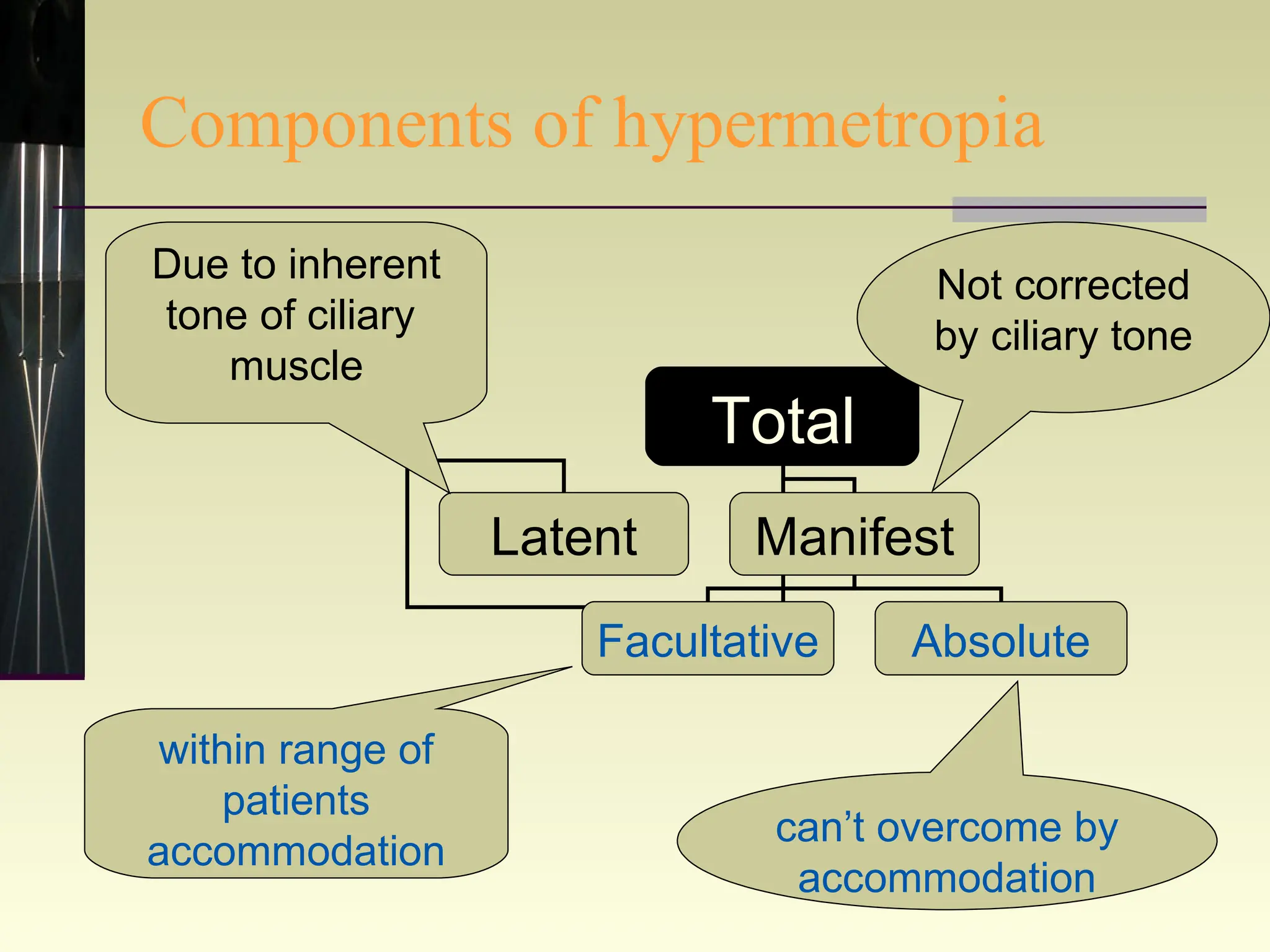
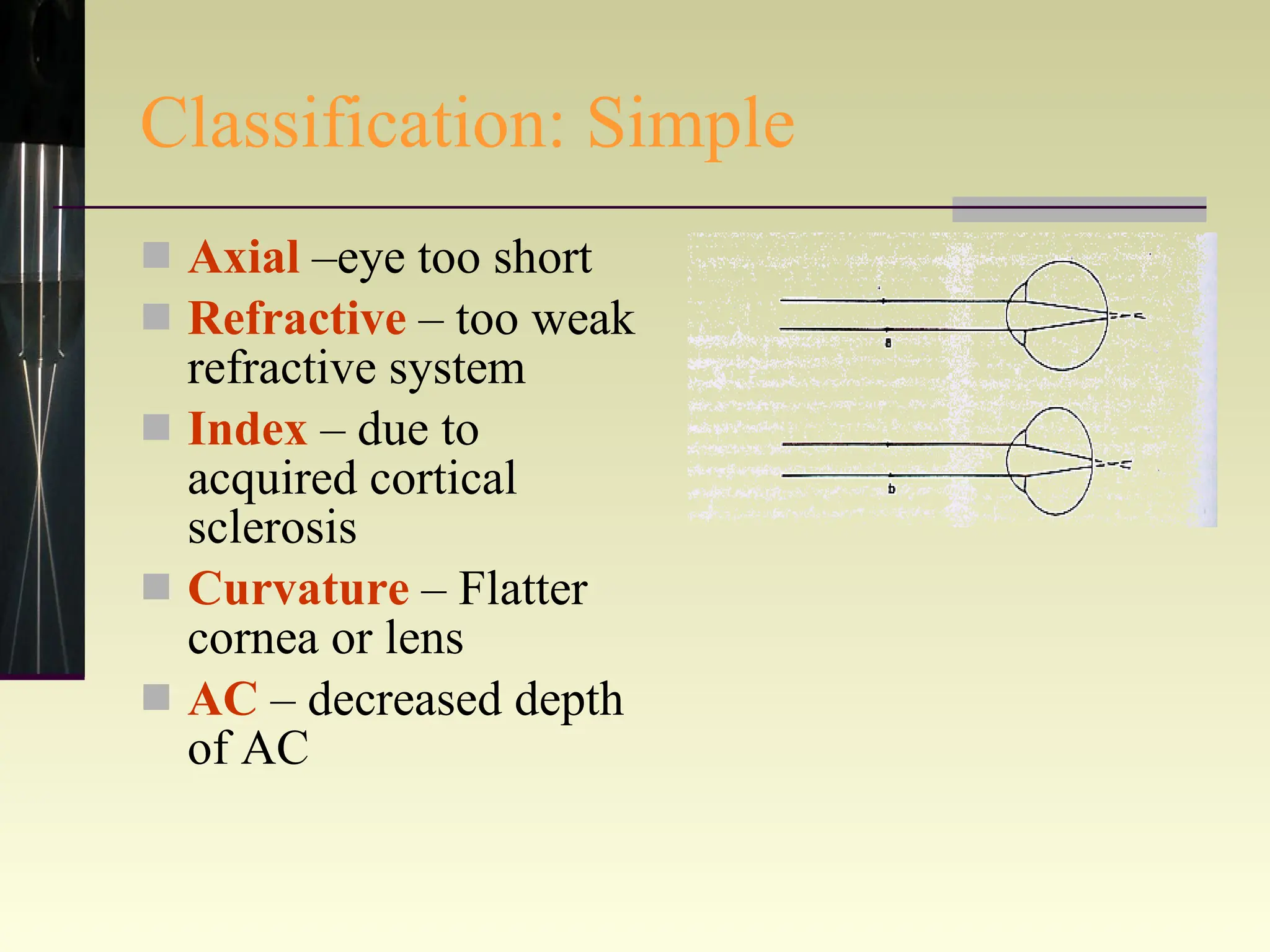
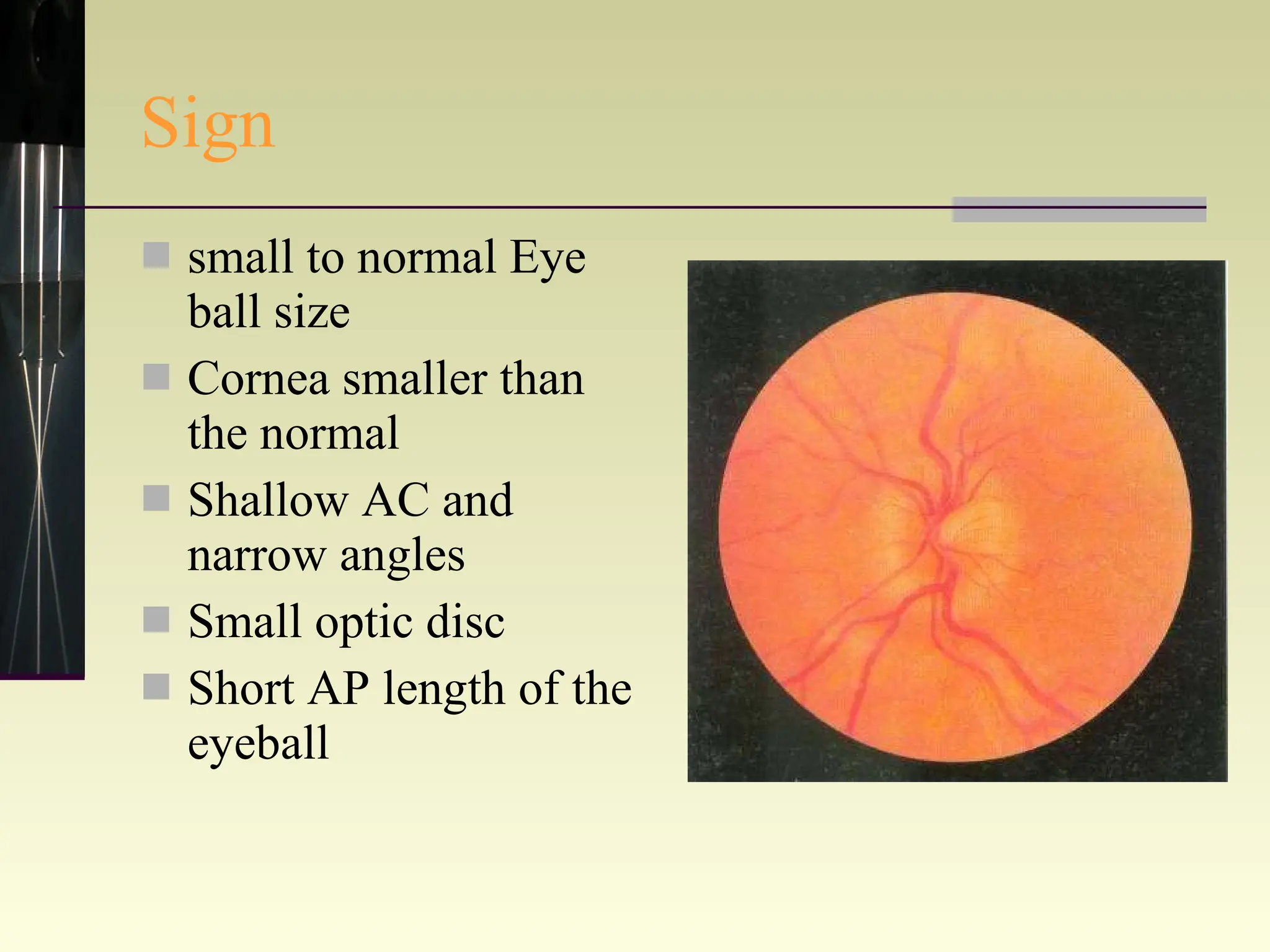
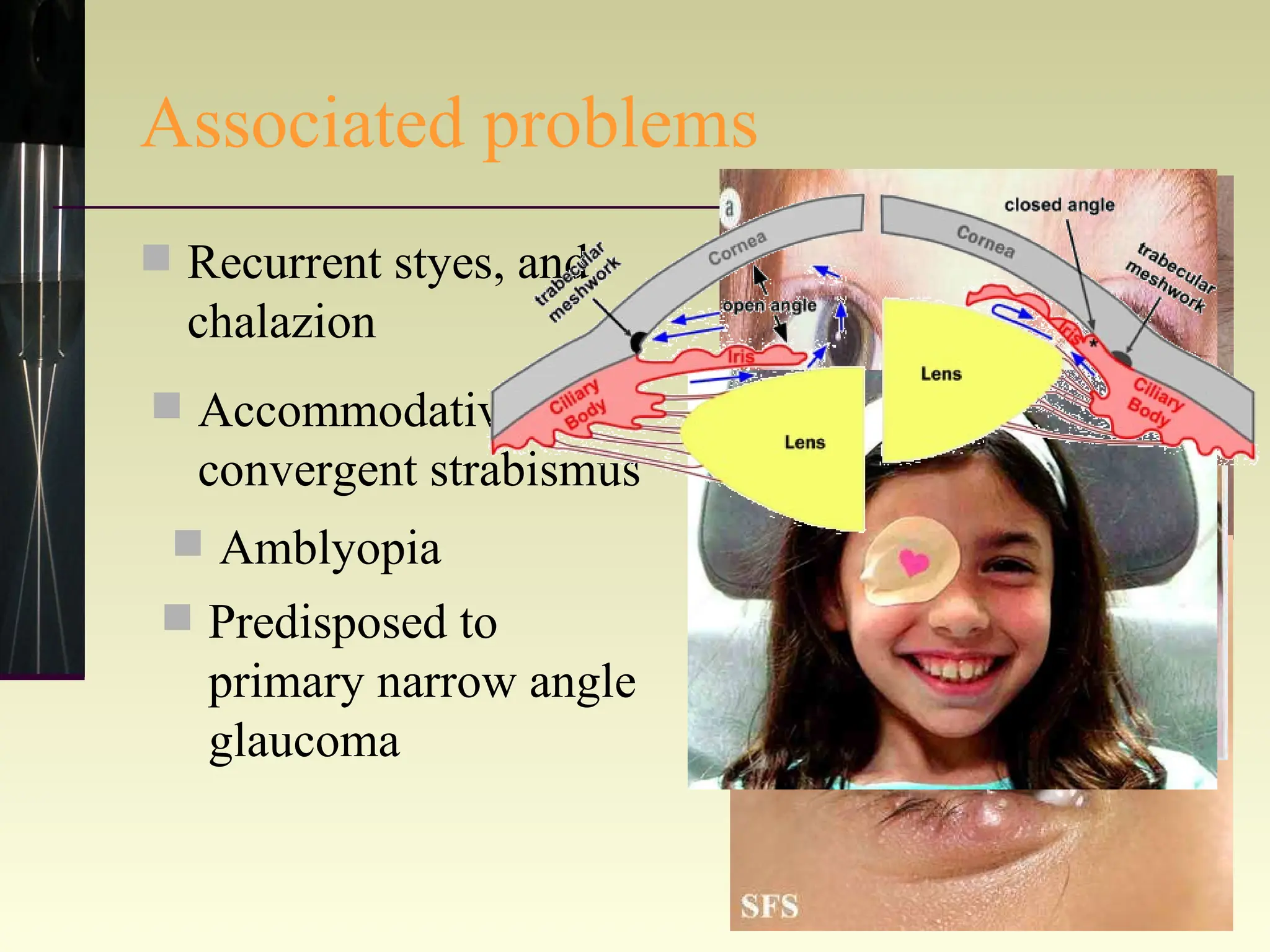
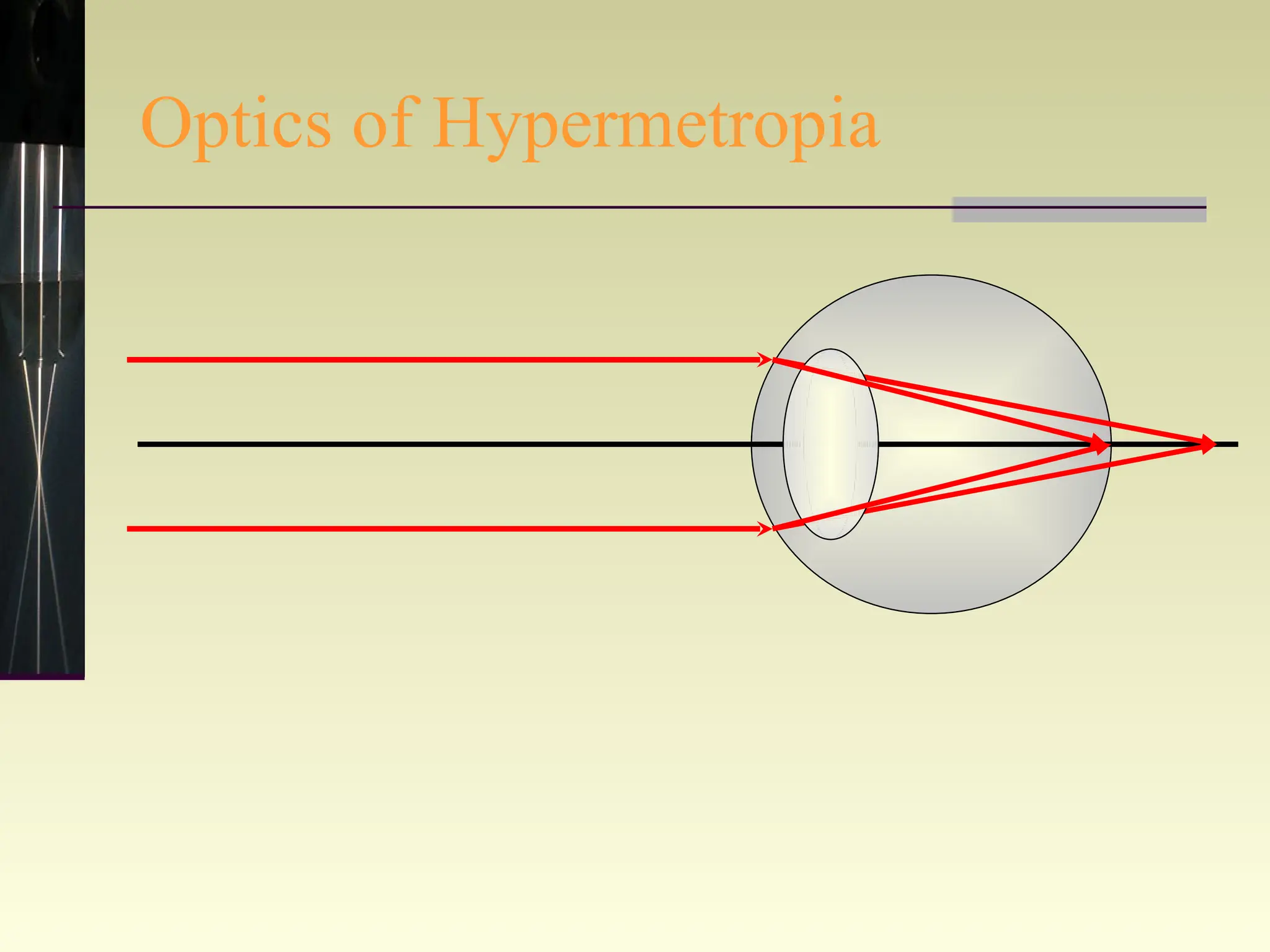
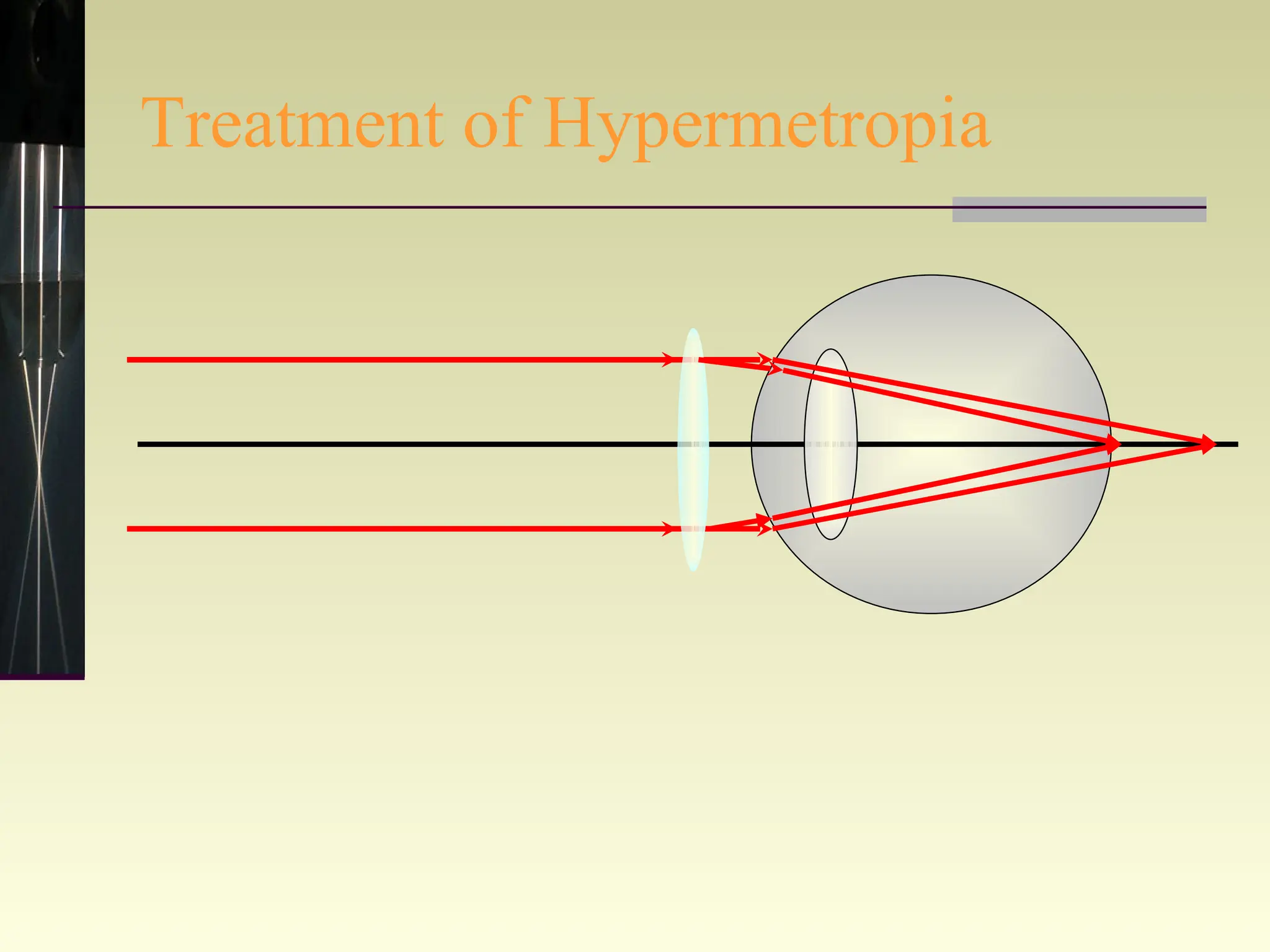
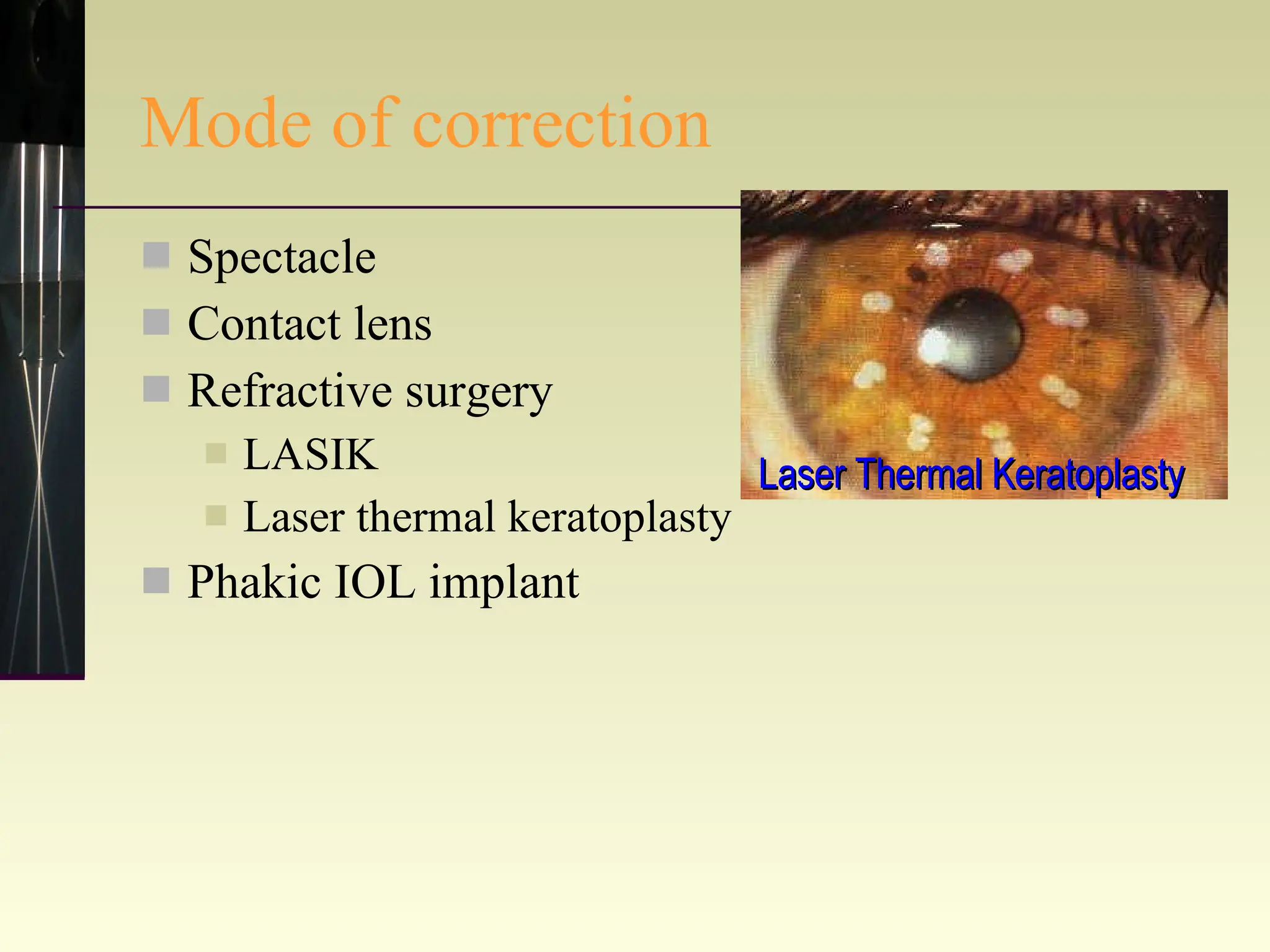

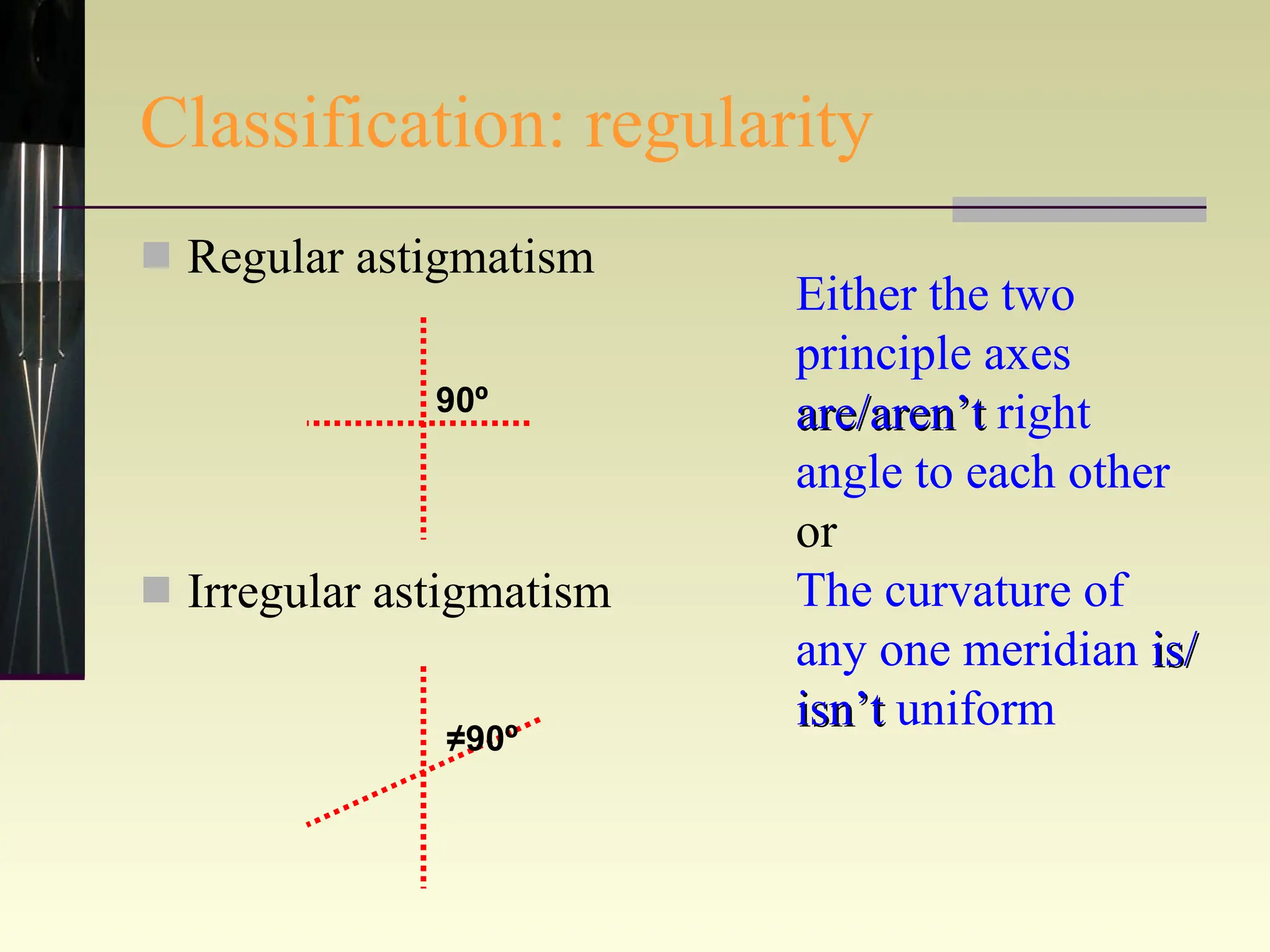
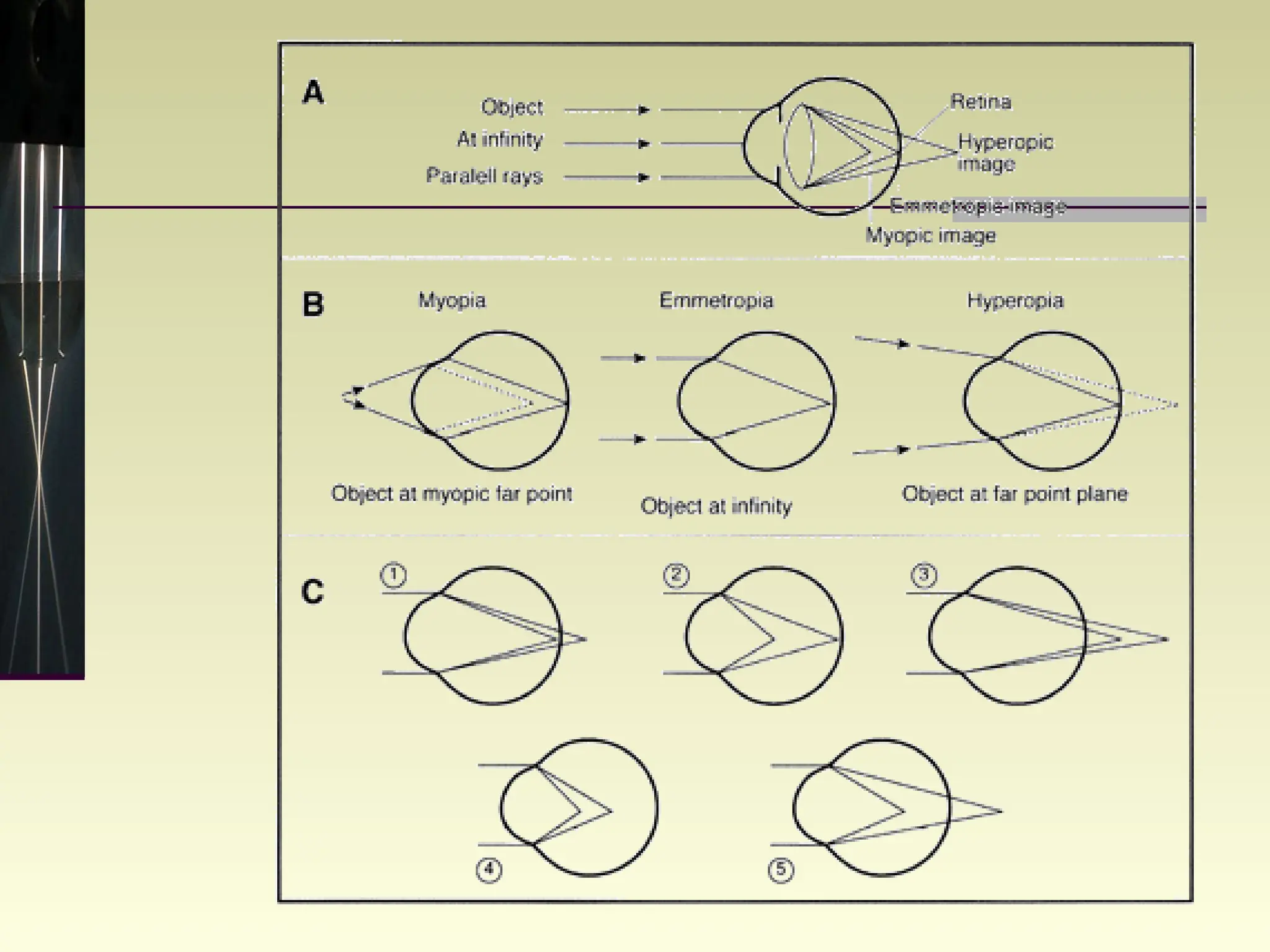


This document summarizes different types of refractive errors including myopia, hypermetropia, and astigmatism. It describes their causes, classifications based on severity and progression, associated signs and symptoms, and methods of correction through lenses, refractive surgery, or other treatments.



































































