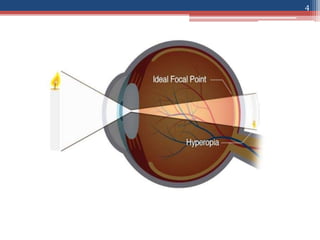
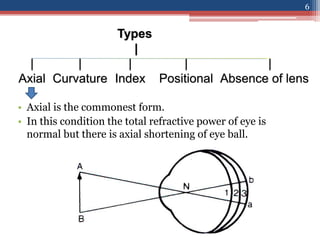
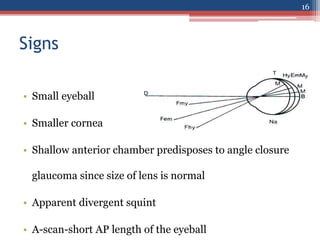
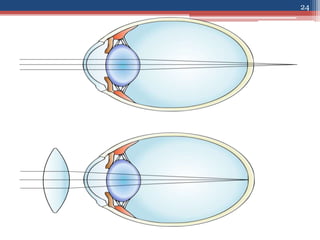
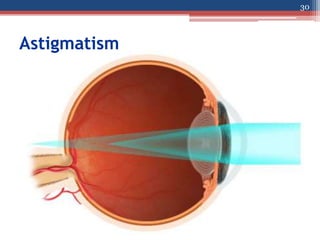
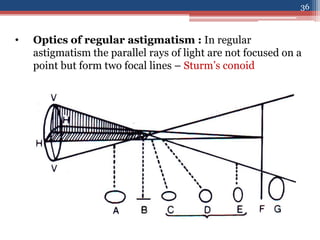
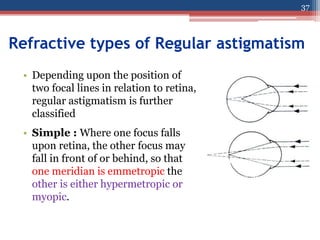
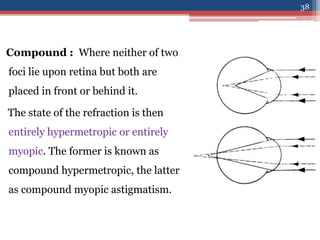
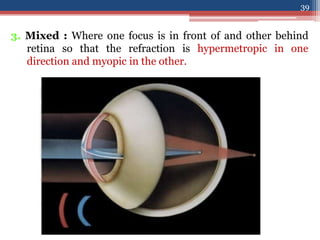
This document discusses different types of optical anomalies of the eye including hypermetropia and astigmatism. It defines hypermetropia as a refractive error where light focuses behind the retina. The causes of hypermetropia include axial shortening of the eyeball or increased curvature of the refractive surfaces. Astigmatism is defined as a refractive error where refraction varies in different meridians, causing blurred vision. Regular astigmatism can be with-the-rule, against-the-rule or oblique, while irregular astigmatism results from corneal scarring. Treatment options discussed include refractive correction with glasses or contacts as well as refractive surgery.



















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



