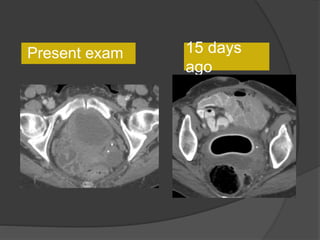
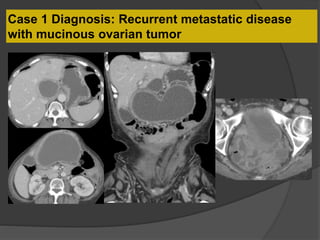
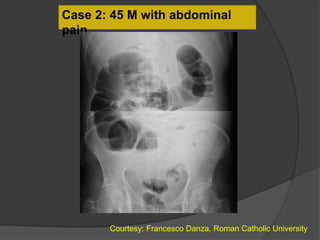
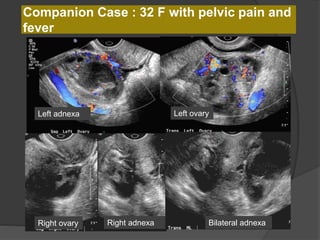
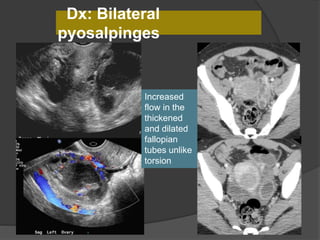
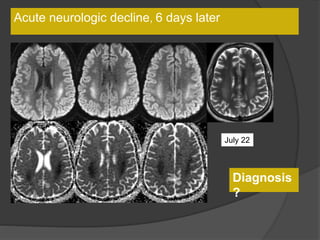
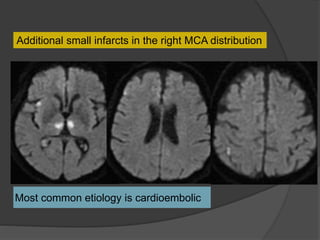
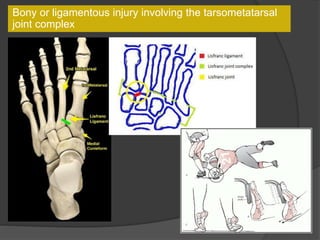
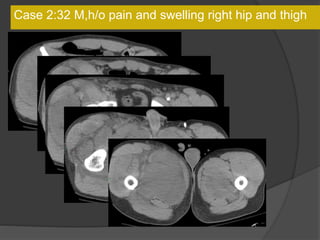
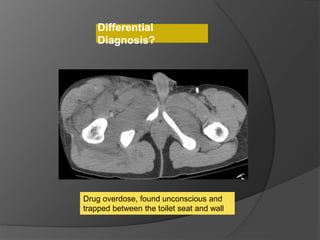
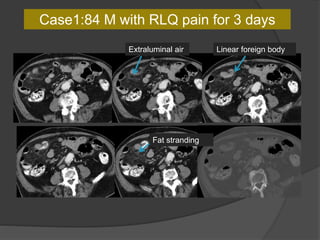
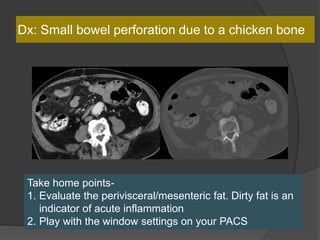
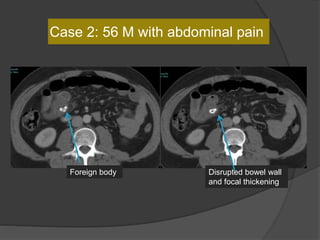
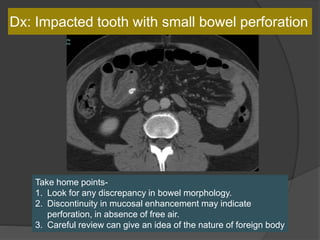
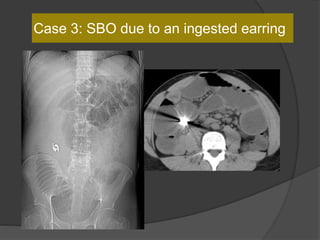
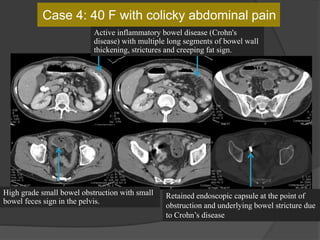
A film reading panel discussed various radiology cases involving abdominal, chest, musculoskeletal, and neurological conditions. Experts provided diagnoses and teaching points for each case, highlighting imaging findings and correlating radiological features with clinical information. A range of pathologies were reviewed including tumors, infections, vascular diseases, and traumatic injuries.